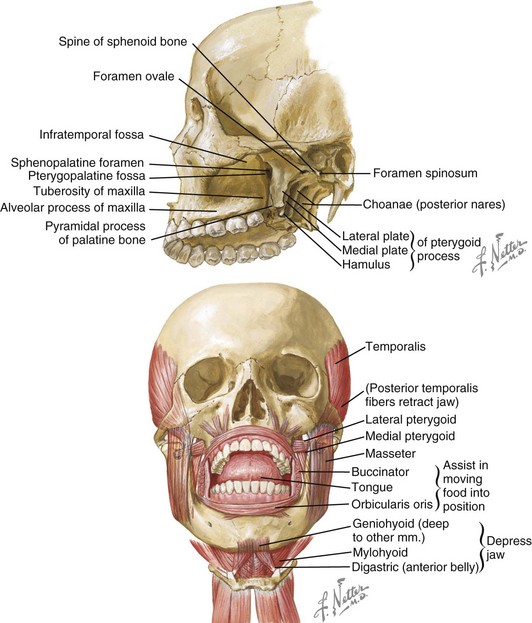
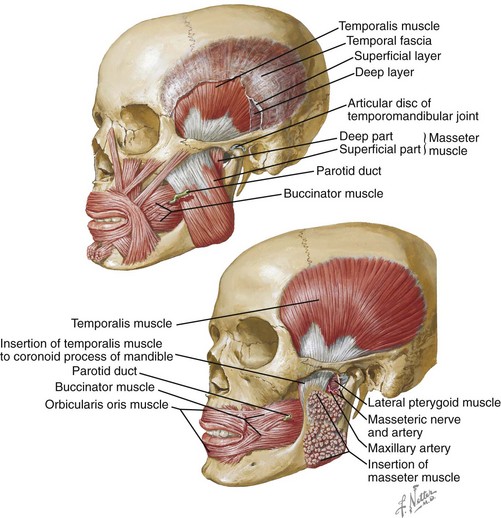
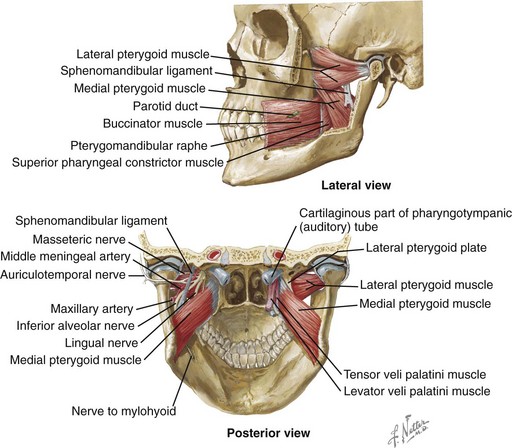
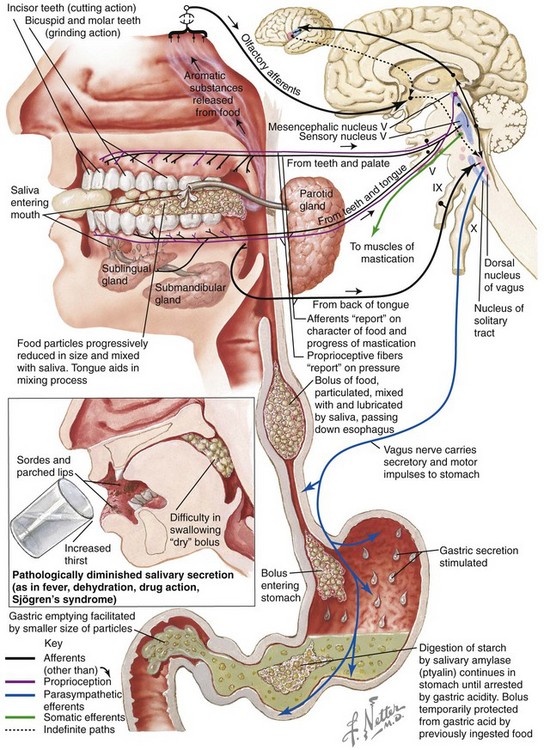
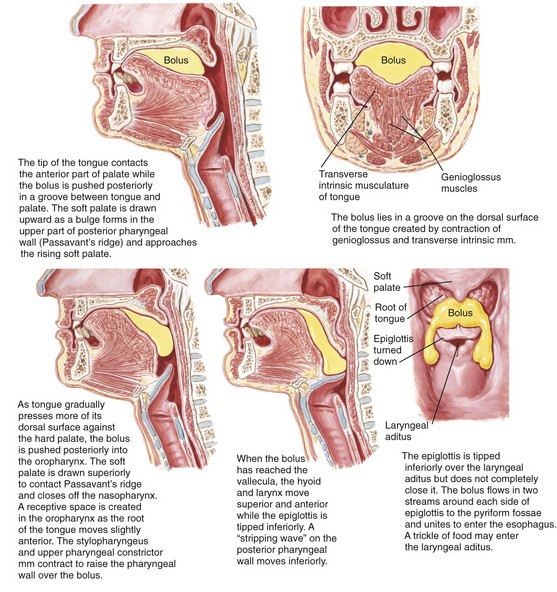
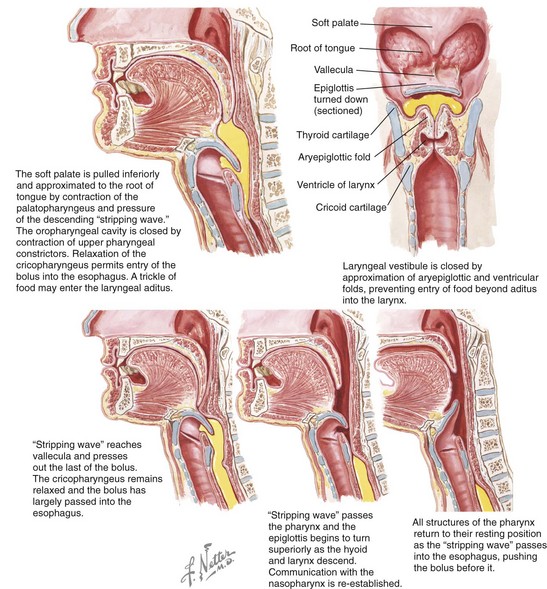
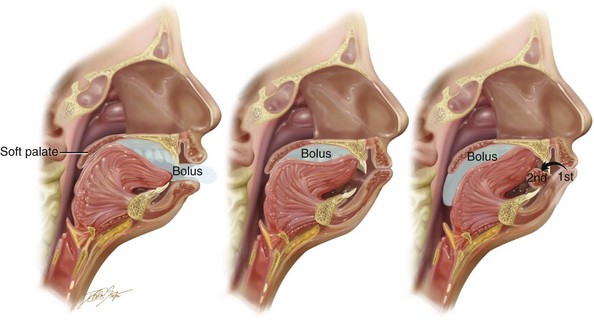
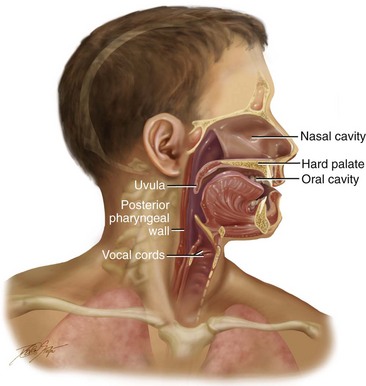
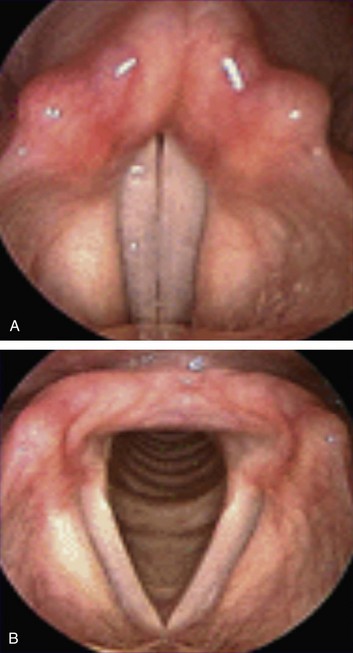
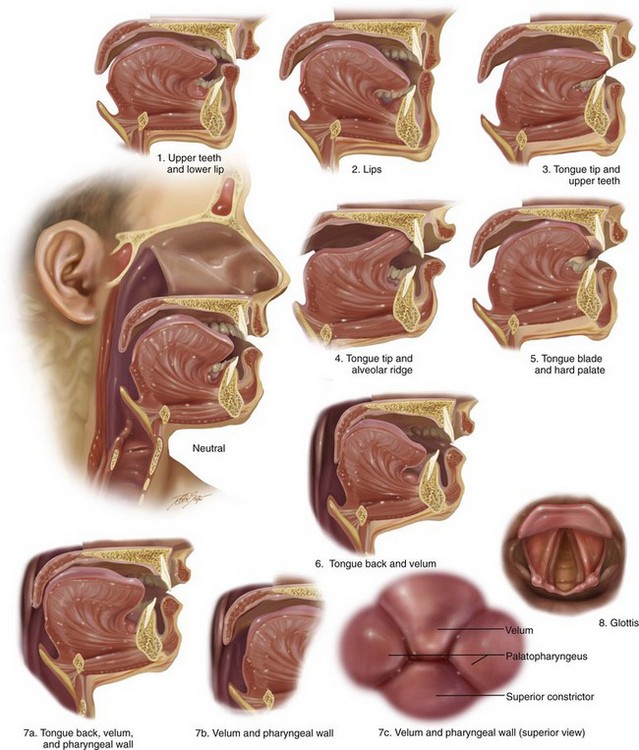
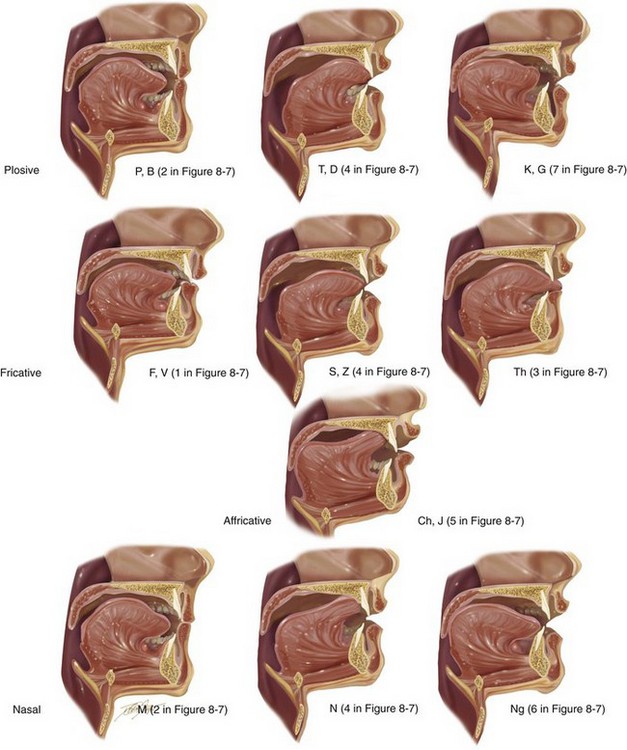
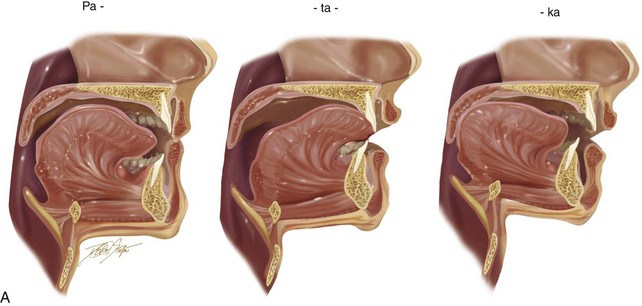
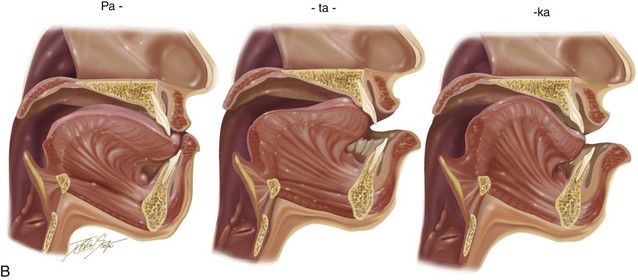
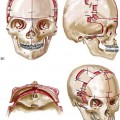
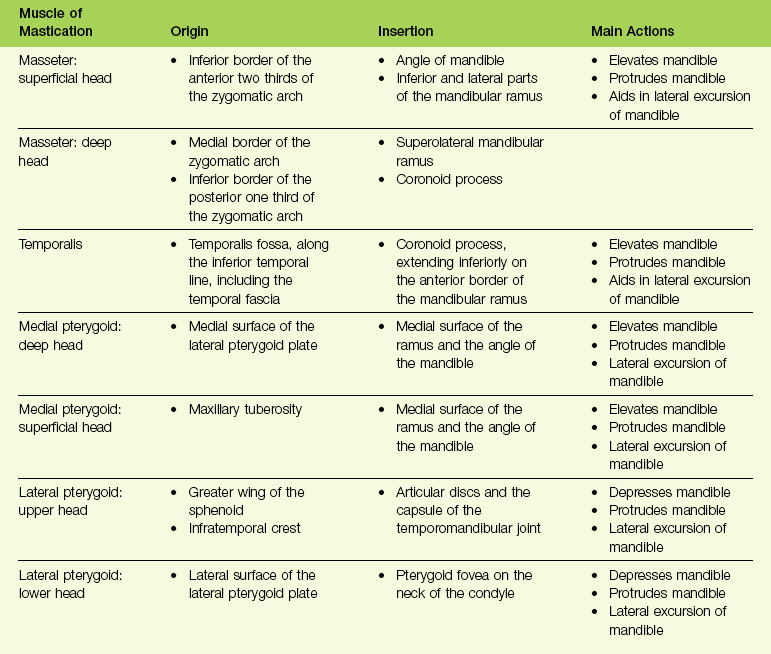
8 The physiologic and functional mechanisms of human speech, mastication, and swallowing are essential for an individual to maintain his or her normal performance levels. These are highly coordinated and complex actions that are closely interrelated. These functions are susceptible to physical impairments, such as the presence of a dentofacial deformity. This chapter will review the mechanisms of normal speech, mastication, and swallowing. The potential for negative sequelae that stem from the presence of a jaw deformity with malocclusion and the benefits of successful reconstruction are also reviewed.11,151 The masticatory system is an integrated complex that is primarily made up of bones, muscles, ligaments, and teeth. Movement of the structures is neurologically coordinated for efficient function and for the maintenance of the component parts over the individual’s lifetime.1–3 Controlled contracture and relaxation of the head and neck musculature are necessary to move the mandible, the soft palate, the lips, and the tongue efficiently for effective function (i.e., speech, swallowing, and chewing). A neurologic control system regulates and coordinates the activities of the entire masticatory system. The dynamic balance of muscles in the head and neck is made possible through feedback that is provided by sensory receptors.10 To create a precise mandibular movement, input from the various sensory receptors is received by the central nervous system through the afferent fibers.41 The brain stem and cortex work together to assimilate and organize this input, and then provide modulated motor activities through the efferent nerve fibers.80 Within the brain stem, neurons control rhythmic muscle activities for effective breathing, swallowing, and chewing.25 These neurons are called the central pattern generator (CPG).96 The CPG is responsible for the timed and integrated activity among antagonistic muscles that is needed to accomplish these functions. For example, during chewing, the suprahyoid and infrahyoid muscles contract at the same time that the elevator muscles relax; this allows the mouth to open and accept food. With the bolus of food in the mouth, the CPG causes contraction of the elevator muscles while relaxing the suprahyoid and infrahyoid muscles, thereby producing closure of the mouth onto the food bolus. This chewing mechanism is repeated until the particles of food are small enough to be efficiently swallowed. All of this assumes that the individual has normal functioning of the tongue and lips, adequate numbers and locations of teeth, and intact temporomandibular joints and jaws (Fig. 8-1).43 Ideally, with all of these component structures in place, chewing can be accomplished without excess stress to any of the component parts. Although chewing is typically a subconscious activity, it can be brought into conscious control at any time. Likewise, breathing and swallowing are generally carried out as subconscious activities, but they can also be brought under voluntary control to be refined (Table 8-1). Figure 8-1 Mastication is the process of chewing food in preparation for deglutition (swallowing) and digestion. All muscles of mastication originate on the skull and insert on the mandible. All muscles of mastication are innervated by the mandibular division of the trigeminal nerve. All muscles of mastication are derivatives of the first pharyngeal arch. Movements of the mandible are classified as follows: The bones involved include the base of the skull and the mandible. The skull base and the mandible articulate at the temporomandibular joint between the squamous portion of the temporal bone and the condyle of the mandible. Netter illustration from www.netterimages.com © Elsevier Inc. All rights reserved. Mastication is defined as the act of chewing food (Fig. 8-2). It represents the initial stage of digestion. During mastication, the food bolus is broken down into small particles for ease of swallowing. For most, it is considered an enjoyable activity that involves the senses of taste, touch, and smell. It is a complex function that requires the involvement of the muscles, the teeth, and the periodontal supportive structures. It also requires functioning temporomandibular joints and jaws, and it makes use of the lips, the cheeks, the tongue, the palate, and the salivary glands. It is an activity that is usually automatic and often taken for granted, although it can be easily brought into voluntary (i.e., conscious) control. It is also susceptible to pathologic conditions and damaging habits. Furthermore, modifications of this system (i.e., compensatory patterns) will be introduced when component parts are not in proper working order (e.g., in the presence of dentofacial deformity with malocclusion). Figure 8-2 Mastication prepares food via “chewing” for deglutition and digestion. The illustrations and legends show an overview of the process. Netter illustration from www.netterimages.com © Elsevier Inc. All rights reserved. In the normal setting, mastication is made up of rhythmic, well-controlled separations and closures of the maxillary and mandibular teeth. This activity is under the control of the CPG, which is located in the brain stem. Each opening and closing movement of the mandible represents a chewing stroke.79 The chewing stroke can be divided into the opening phase and the closing phase. The closing phase may be further subdivided into the crushing phase and the grinding phase. During mastication, the chewing stroke is repeated until the food is broken down into small enough parts for swallowing. After the food has been incised (usually with the anterior teeth) and then brought further into the mouth, the crushing of the bolus is concentrated on the posterior teeth. It has been documented that the tooth contact ability, the number of teeth, and the quality of the teeth influence the chewing stroke. During mastication, sensory information is sent back to the central nervous system.5,158 This feedback mechanism allows for the alteration of the chewing stroke in response to the particular food being chewed and the quality of the anatomic structures that are available for chewing.65 Generally, with maximum full intercuspation (i.e., tall cusps, deep fossae, and ideal contacts), a predominantly vertical chewing stroke is seen. When there is a flattened occlusal surface (e.g., as a result of occlusal equilibrium or a grinding habit that involves a loss of enamel), a broader chewing stroke can be documented.54,81 The presence of malocclusion may produce irregular and less repeatable chewing strokes in the individual.6 Studies document that, in approximately 75% of subjects, there is a preferred chewing side.6 Chewing activities normally occur on the side with the greatest number of pain-free tooth contacts noticed during lateral glide. The maximum biting force that can be applied to the teeth varies from individual to individual.156 With tougher foods, chewing preferably occurs predominantly on the first molar and second premolar areas. In general, males can bite more forcefully than females. Typically, in the presence of normal anatomy, the maximal amount of force applied to a molar is several times that which can be applied to an incisor.60 The maximum biting force generally increases with age, up to adolescence. Nevertheless, the amount of force placed on the teeth during mastication varies greatly from individual to individual.103,114 When food is introduced into the mouth, the lips must guide and control intake. After the food is in place, the lips must seal off the oral cavity. The lips are especially necessary when liquid is being introduced.58 This is more difficult for the individual with a long face growth pattern that causes mentalis strain and lip incompetence. When the food is in the mouth, the tongue plays a major role in maneuvering the bolus for sufficient chewing. The tongue typically initiates the process of breaking up the food by pressing the bolus against the hard palate; thus, the presence of an oronasal fistula in a patient with a cleft palate can be problematic. The tongue then pushes the food onto the occlusal surfaces of the teeth, where it can be effectively crushed during the chewing stroke. During the opening phase of the next chewing stroke, the tongue repositions the partially crushed food again onto the teeth for further breakdown. While the tongue is repositioning the food that has been displaced lingually, the buccinator muscle in the cheek region is compressing the food that has shifted into the vestibule back over the molars. The displaced food is continuously repositioned on the occlusal surfaces of the teeth until the particles are small enough to be swallowed efficiently. The tongue is also used to separate the food particles that require more chewing (and are therefore replaced over the molars) from those that are now small enough for swallowing. This sorting process is essential to prevent choking on large food particles. After the eating process is complete, the tongue is used to clean the teeth and to remove any food residue that has been trapped in locations such as the floor of the mouth (i.e., the sulcus) or in the labial vestibule. In the presence of normal anatomy, the ingestion of a bolus of food is made easier by the active lowering of the mandible, the opening of the lips, and the depression of the tongue.25 All of these activities increase the size of the oral cavity to accommodate the bolus that is to be ingested. Not surprisingly, temporomandibular joint ankylosis or masticatory muscle pain with trismus will limit mouth opening and alter the process. The ingestion of fluid is usually via sucking (e.g., with a straw). In this case, the lips remain sealed around the delivery device, and the exit to the back of the oral cavity is closed by the tongue and the soft palate. In the individual with a long face growth pattern (i.e., lip incompetence and an anterior open bite), this will be more difficult. The lowering of the mandible and the depression and retraction of the tongue are accomplished by bracing the cheeks laterally and the mouth floor inferiorly. These actions will generate a subatmospheric pressure within the oral cavity to facilitate the flow of fluids into the oral cavity. This process will be more difficult in the presence of an oronasal fistula (i.e., an incompletely repaired cleft palate). This form of suction is also a useful mechanism for driving the entry of saliva into the oral cavity from the salivary glands.112 Swallowing is a process that occurs through a series of coordinated muscular contractions that move the bolus of food from the oral cavity through the esophagus and into the stomach (Fig. 8-3). It requires voluntary, involuntary, and reflex muscular activity. The decision to swallow generally depends on the following: (1) the degree of fineness of the food (2) the intensity of the taste extracted and (3) the degree of lubrication of the bolus. During the swallowing mechanism, the lips are closed to seal the anterior aspect of the oral cavity. The teeth are brought into their maximum intercuspal position for the stabilization of the mandible. With the mandible fixed, the contraction of the suprahyoid and infrahyoid muscles will control the movement of the hyoid bone for effective swallowing. Figure 8-3 Deglutition or swallowing is a combination of voluntary and involuntary muscle contractions that move a bolus of food from the oral cavity to the esophagus. These illustrations review the details of the process. Netter illustration from www.netterimages.com © Elsevier Inc. All rights reserved. In the normal growing child, as the posterior teeth erupt, the occluding teeth are able to brace the mandible, and the transition to an adult swallow occurs. In the presence of malocclusion, either from a developmental jaw deformity (i.e., an anterior open bite or a Class II malocclusion with significant overjet) or from the loss of teeth from either tumor or trauma, the infant swallow is maintained or reassumed (Fig. 8-4). In the presence of an anterior open bite, it is necessary for the individual to thrust the tongue forward to close the gap during the swallowing mechanism. This is an appropriate compensatory swallowing pattern. Figure 8-4 Illustrations of a compensatory swallowing mechanism in an individual with a Class II excess overjet malocclusion. This illustration is representative of the patient shown in Figure 8-10. Studies confirm that this repetitive swallowing cycle occurs approximately 600 times during a 24-hour cycle in the average individual.33 The general breakdown includes cycles during eating, cycles between meals while awake, and cycles during sleep. Lower levels of salivary flow during sleep result in less need for swallowing.112 The mechanism of speech is composed of several highly integrated processes (Fig. 8-5)26,31,122: Figure 8-5 Illustration of a cross section through the head and neck that shows the pertinent anatomy required to articulate speech. • Speech initiation, during which the content of the utterance to be spoken is converted into phonemes in the brain’s language center • The generation of commands that go from the brain’s motor center to the speech organs • Phonation, during which the emission of air sent from the lungs moves through the vocal tract and causes the formation of the voice as it moves past the vocal folds • Articulation, which involves movement by the oral cavity, the oral pharynx, and the hypopharynx for the production of speech via this specific set of motor commands During human speech production, the airflow that is sent from the lungs with a constant pressure passes between the vocal cords; the vibration of the vocal cords causes the airflow to be converted into cyclic puffs of air that then become sound (Fig. 8-6). The airstream is interrupted by movements of the jaws, the tongue, the soft palate, and the lips. These movements change the shape of the vocal tract, which in turn enables the individual to control the articulated sound and resonance characteristics.4 The pitch of the voice changes in accordance with adjustments that are made in the tension of the vocal cords. Voiced sounds incorporate the vibration of the vocal cords in addition to the placement of the articulators. Unvoiced sounds are produced by the interruption of the airstream by the articulators. Voiced sounds are produced with vocal fold vibration that accompanies articulator placement. Vocal tract resonance characteristics are controlled by the cross-sectional area of various parts of the vocal tract.36 Examples include the articulation of the upper lip to the lower lip for the bilabial sounds of /p/, /b/, and /m/ and the articulation of the tongue to the alveolar ridge for the production of the lingual-alveolar sounds /t/, /d/, /n/, /l/, /s/, and /z/.120 Figure 8-6 A view of vocal cords as seen via nasoendoscopic examination. A, Closed vocal cords (adduction position). B, Open vocal cords (abduction position). Individual articulators (i.e., upper jaw, lower jaw, upper lip, lower lip, tongue, soft palate, hard palate, upper teeth, and lower teeth) are used for both the speech mechanism (Figs. 8-7 and 8-8; Table 8-2) and for the mastication and swallowing (deglutition) mechanisms (see Figs. 8-1, 8-2, and 8-3).123 Speech sounds are composed of the approximation of individual articulators within the speech mechanism and the manner in which the airflow from the vocal cords is modulated.59 This in turn produces what is called a phoneme, which is known to most as an isolated speech sound. A significant feature of articulatory movements is the phenomenon of assimilation in which the mouth position for an individual phoneme in the utterance incorporates the effects of the mouth position for the phonemes uttered immediately before and after. Interestingly, a human can imitate the sound of an utterance that he or she has heard without necessarily being able to speak the language of the utterance.66 In other words, the individual can estimate which mouth movements are necessary to produce a sound that is similar to the one that he or she has heard. By convention, the classification of speech sounds is categorized in accordance with their manner and place of production (i.e., the location of articulation). TABLE 8-2 Kinesiologic Positions for the Oral and Pharyngeal Musculature during the Articulation of Speech Sounds Figure 8-7 Diagram showing the kinesiologic positions for the oral and pharyngeal musculature during the articulation of speech sounds. Figure 8-8 Illustrations that demonstrate the articulation of sounds created by specific positions of the lips, tongue, and teeth in the presence of harmonious jaws and occlusion. The numbering allows you to refer back to the chart shown in Figure 8-7, B, to correlate the anatomic position of the articulators with the associated speech sounds. Vocal tract variables include the dynamic voluntary movements of the vocal organs (e.g., lower jaw, tongue, soft palate, vocal cords, upper lip, lower lip); these organs and their movements are influenced by the basic positions of the organs in relation to each other. The baseline position of the jaws and teeth vary widely; however, if they are significantly displaced (i.e., if there is malposition of the teeth or jaws), this can negatively affect articulation (Fig. 8-9). When the position of a jaws is abnormal (i.e., dentofacial deformity) and then successfully corrected via orthodontics and orthognathic surgery, including a return of normal morphology, then the tongue may or may not respond instantaneously to achieve a more normal utterance of specific consonant or vowel sounds (see Fig. 8-8). Figure 8-9 A, Drawings that show the representative stages of lip, dental, and tongue positioning during the production of the word patty-cake. B, In the presence of a jaw deformity with malocclusion, the lips and tongue must position themselves in other locations (i.e., via compensatory mechanisms) to create similar sounds in an attempt to achieve effective communication. This is demonstrated in an individual with a long face Class III negative overjet anterior open-bite malocclusion and similar to what is seen in the patient in Figure 8-11. Speech sounds are generally divided into the categories of consonant sounds and vowel sounds. The production of consonant sounds requires the obstruction or partial closure (i.e., sphinctering) of the airstream at specific sites along the vocal tract.121 The classifications of consonant sounds are based on the extent of airstream obstruction, the site of airstream obstruction, and whether the vocal cords vibrate.16,17 Vowel sounds are generally produced by the position of the tongue and lips without airstream obstruction and with the upper and lower teeth more widely separated. All vowel sounds are voiced, and it is for this reason that vowel sounds are generally less affected by the malpositioning of the teeth or jaws than consonant sounds are.138 • Plosive/stop: Air pressure is stopped within the oral cavity at a specific location, and it is then suddenly released. Examples are /p/, /b/, /t/, /d/, /k/, and /g/. • Fricative: Air pressure is partially blocked or obstructed within the vocal tract, thereby causing turbulent airflow. Examples are /f/, /v/, /s/, and /z/. • Affricative: There is a sequencing of the airstream initially with complete obstruction (i.e., plosive/stop) followed by fricative (i.e., partial vocal tract obstruction) at the same location. Examples are /ch/ and /j/. • Nasal: Air is allowed to pass freely through the nasal cavity. Examples are /m/, /n/, and /ng/. The anatomic locations of the vocal organs that block or partially block the airflow (i.e., places of articulation) include the following: bilabial (upper lip to lower lip); labiodental (lower lip to upper teeth); interdental (tongue between the upper and lower teeth); lingual to palate alveolar (tongue to alveolar process of the upper jaw), lingual to palate (tongue to hard palate); and glottal (vocal cords to each other).124 The assessment of speech disorders involves the use of a number of tests and techniques.23,24,27,32,34,75,109,132,139 Historically, various tests have been described to assess speech and how it compares with recognized normative values. These assessments typically will evaluate sound production in the word position or within sentences. Tests that are frequently used for the assessment of speech are found in Box 8-1. These tests are based on determining errors when the results are compared with those of normal individuals during single-word utterances. The Bzoch Error Pattern Diagnostic Articulation Test further grades each error type in accordance with its severity. All of these tests fall short for the assessment of the complexities of dynamic speech. Among educators and clinicians, there is often a lack of agreement with regard to a preferred objective method for the analysis of speech. The majority of the published studies were carried out to analyze the effects of orthodontics and orthognathic surgery on speech attempt to document articulation error rates in a traditional manner by noting sound production as simply correct or incorrect and by noting substitutions, distortions, or omissions. Some studies further describe errors as either visual or auditory in an attempt to overcome the usual problems associated with detecting mild sibilant distortions that might not be captured on audiotape.161 The classic negative effects of a jaw deformity with malocclusion on speech articulation are known.30,35 The speech benefits of successful orthodontic and surgical correction will have their most notable effects on consonant articulation within the fricative class, which includes /s/, /z/, and /f/. It is known that the /s/ sound in particular is highly sensitive to precise tongue placement and to the accurate direction of airflow across the incisal edges of the upper and lower teeth. The characterization of speech error type is usually defined as follows: • Substitution: when one sound is replaced by another • Omission: when a sound is omitted from a word altogether • Distortion: when sound is not produced appropriately but is still understood • Visual distortion: when the visual appearance of making the sound is abnormal but the sound itself is correct • Auditory distortion: when the perception of the sound (what is heard) is abnormal but the appearance (visual appearance) of the positioning of the anatomy is correct • Combined visual/auditory distortion: when both the perception of the sound and the appearance of the production of the sound are abnormal Published studies show a tendency for individuals with Angle Class I occlusions to rate better with regard to speech as compared with those individuals with malocclusions.37 A review of the literature shows a significant association between misarticulation in speech and Angle Class II malocclusion (Fig. 8-10), Angle Class III malocclusion (Fig. 8-11), and anterior open-bite malocclusion (Fig. 8-12).39,43,53,54 Studies that evaluate speech articulation in individuals with jaw deformity and malocclusion confirm that as many as 90% of affected individuals have significant misarticulation errors. Several published studies report articulation errors among all jaw deformity patients analyzed.39,47,53 Figure 8-10 A 16-year-old girl arrived with her parents for the surgical evaluation of a developmental jaw deformity with malocclusion. She was diagnosed with a primary mandibular deficiency, a maxillary arch constriction, and a Class II excess overjet growth pattern. Attempts at orthodontic growth modification and camouflage in the past were unsuccessful. There was a lifelong history of obstructed nasal breathing, heavy snoring, and the suggestion of sleep apnea. The patient experienced difficulty with chewing, swallowing, speech articulation, breathing, and lip closure/posture. A formal evaluation by a speech–language pathologist was carried out. • Difficulty with chewing solid, textured food • Only able to chew on the back teeth • Frequently swallows foods partially whole, especially raw vegetables and meat • Normal to mild labial weakness during repeated puckering and retraction tasks • Lingual range of motion within normal limits • Assessed via the Fisher-Logemann Test of Articulation and informally during speech and conversation • Misarticulations were identified, including /s/, /sh/, /st/, /z/, /dz/, and /sk/
Speech, Mastication, and Swallowing Considerations in the Evaluation and Treatment of Dentofacial Deformities
The Neuromuscular Masticatory System
The muscles involved in the masticatory process include four paired muscles:
Mastication Mechanism
Swallowing Mechanism
Speech: Mechanism, Formation, and Assessment

Effects of Jaw Deformities with Malocclusion on Speech
Background



Chewing/swallowing:
Related posts:
![]() Temporomandibular Disorders: Effects of Occlusion, Orthodontic Treatment, and Orthognathic Surgery
Temporomandibular Disorders: Effects of Occlusion, Orthodontic Treatment, and Orthognathic Surgery
 Treacher Collins Syndrome: Evaluation and Treatment
Treacher Collins Syndrome: Evaluation and Treatment
![]() Long Face Growth Patterns: Maxillary Vertical Excess with Mandibular Deformity
Long Face Growth Patterns: Maxillary Vertical Excess with Mandibular Deformity
![]() Primary Mandibular Deficiency Growth Patterns with or without Maxillary Arch Constriction
Primary Mandibular Deficiency Growth Patterns with or without Maxillary Arch Constriction
 Maxillary Deficiency with Relative Mandibular Excess Growth Patterns
Maxillary Deficiency with Relative Mandibular Excess Growth Patterns
 Syndromes with Craniosynostosis: Evaluation and Treatment
Syndromes with Craniosynostosis: Evaluation and Treatment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Speech, Mastication, and Swallowing Considerations in the Evaluation and Treatment of Dentofacial Deformities
 Note:
Note: 