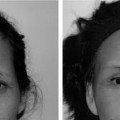
9 The Asian nose differs from that of the Caucasian in fundamental respects: the cartilage tends to be weaker and in short supply for grafting, the skin envelope is much thicker, and the nose is typically underprojected and the tip, amorphous. Given these dissimilarities, an entirely different strategy than traditional Western rhinoplasty must be envisioned for the Asian nose to achieve the intended aesthetic objectives.1,2 The primary method for augmentation rhinoplasty of the Asian nose is silicone implantation, which has remained a steadfast and safe material for rhinoplasty in Asia. Because Chapter 3 has already outlined a systematic approach to rhinoplasty using this method, this chapter will focus instead on specialized topics concerning this subject in greater detail. Besides augmentation of the tip and dorsum with a silicone implant, other ancillary procedures may benefit the Asian nose as well. The premaxillary component tends to be underdeveloped in the Asian nose, leading to an acute nasolabial angle that imparts an unaesthetic simian-like appearance to the nose-lip complex. The author does not favor use of an extended silicone implant that spans the entire columellar distance to address this deficiency: this type of implant risks extrusion and may contribute to pressure necrosis of the nasal tip. Instead of pushing the nose forward with this unfavorable “tent pole” type of implant, a separate premaxillary implant should be fashioned that can improve the nasolabial angle. Premaxillary augmentation is covered in detail in Chapter 11 on facial implants. Another aspect of the Asian nose that imparts an overly ethnic appearance, which cannot be addressed with a silicone implant alone, is a wide alar base. Flared nostrils are particularly prevalent in the darker complected Polynesian races but is found to some extent in almost all Southeast Asian ethnicities. Alar-base reduction may effect a more favorable tip configuration in select Asian patients. Oftentimes, the alar base appears to be overly wide only because the nasal tip is relatively underdeveloped. Tip enhancement alone with a silicone implant may be sufficient to achieve the desired balance of the nasal tip vis-à-vis the side alae. This chapter will discuss both the aesthetic criteria that should be followed to determine the candidacy of a prospective patient for alar-base reduction and the technical details on proper surgical technique. Although augmentation of the nasal tip and dorsum serves as the primary directive in Asian rhinoplasty, not all Asian noses follow this precise model. In particular, the Japanese nose stands in contradistinction to other Asian ethnicities in its shape and contour that mandates an alternative surgical strategy. The nasal dorsum appears to be at times overly projected and even may exhibit a dorsal convexity similar to the Caucasian nose, whereas the tip may remain retruded and ill-defined like the typical Asian nose. A combination of Western and Asian techniques should be exercised to address this nasal configuration. A systematic approach will be outlined for noses that tend to exhibit a mixture of leptorrhine and mesorrhine features. It should be emphasized that not all Japanese noses exhibit these characteristics, which may also be commonly found in other Asian ethnicities as well. Considering the increasing rise of interracial unions, a judicious selection of Western and Asian techniques may need to be employed for noses of a mixed heritage. Although augmentation rhinoplasty of the Asian nose with silicone is a very safe and reliable method, complications may arise that are unique to this type of rhinoplasty. Like breast augmentation with silicone implants, the nasal tip may undergo contraction over time, usually due to repeated insertions or bouts of infection. Contraction of the nose may also occur idiopathically. Nevertheless, this complication may be a relatively difficult entity to treat and may require unique surgical strategies, which will be set forth in this chapter. Depending on the degree of contraction, the nose may be addressed in a relatively straightforward manner or may require more elaborate techniques to rectify the problem. The decision to undertake an alar-base reduction is contingent upon several factors: a careful analysis of the patient’s nasal and facial features, an investigation of the patient’s aesthetic motivations, and a review of the postoperative course. Although many patients may seem like suitable candidates for this type of surgery, only a select few will meet all of the criteria to justify alar-base reduction (Fig. 9-1A-H). The lower third of the patient’s nose should be studied assiduously to determine the patient’s eligibility for alar-base reduction. Oftentimes, the nasal width appears to be overly wide simply because the nasal tip is retruded and amorphous. Augmentation rhinoplasty with a silicone implant can restore the balance between the nasal tip and the alae, so that alar-base reduction may be unnecessary. Furthermore, if the alae appear to be approximately the same width as the nasal tip preoperatively, alar-base reduction may regrettably serve to accentuate the width of the nasal tip vis-à-vis the narrowed alae rather than improve tip refinement. The patient can be shown this unfavorable outcome by manually pinching the alae together and demonstrating the illusion that the nasal tip increases in width. Accordingly, alar-base reduction should be reserved only for patients who exhibit a greater ala-to-lobule ratio (Figs. 9-2, 9-3). The nose should also be evaluated in the context of the patient’s other facial features. The rule of horizontal fifths may be recalled as a starting point for aesthetic analysis: the nasal width should be roughly equivalent to the width of the patient’s eye (Fig. 9-4). Although this rule is indeed not infallible, it should be thought of as a general guideline. If the surgeon is uncertain how a narrowed nasal base will look for the patient, he or she can again pinch the nasal base until the desired look is achieved. Alternatively, digital morphing can render an easily viewable image for the patient and physician to analyze, with the declared recognition that technology should not be equated with a guaranteed surgical outcome. If a patient has a very wide face, narrowing the nose significantly may create an unbalanced look (Fig. 9-5A-H). As with any rhinoplasty endeavor, the patient’s specific facial features must be thoughtfully assessed when deciding on the proper course of action. Besides being an unaesthetic attribute, wide nostrils that are visible en face may be deemed a sign of bad fortune. Asian patients who subscribe to this cultural folklore believe that very wide nostrils represent a portal through which monetary wealth is drained out. In contradistinction, a high nasal bridge and prominent nose signify wealth and wisdom. These cultural biases that inform patient motivation must be carefully elucidated before surgery should be undertaken. Clearly, an operation that is intended simply to dispel bad omens should be undertaken with caution. An overly rotated nose can expose the nostril aperture excessively, but derotation of the nasal tip with a nasal implant will not decrease nostril show significantly. Even alar-base reduction may not satisfy the patient, as the nostrils will remain visible despite some reduction in overall width. As suggested, visible nostrils may not indicate the presence of a wide alar base but instead that of an overly rotated nose. Accordingly, alar-base reduction would only exacerbate the nasal tip appearance in this condition, as stated before. Finally, if the patient’s motivation is appropriate, and the aesthetic objective is favorable, the patient must still be instructed thoroughly about the postoperative course. Typically, augmentation rhinoplasty with silicone offers a relatively abbreviated recovery period, lasting only several weeks in length. However, alar-base reduction requires an external incision that may remain conspicuous for many months, a fact that should be clearly articulated to the patient. Given the predilection for Asian skin to respond unfavorably to injury, the patient should be fully cognizant of the potential for a longer recovery. The author contends that any external incision on the central aspect of the Asian face risks being visible for a prolonged period of time. Unlike a face lift or brow lift incision that is hidden away near the hairline, an external nasal incision may draw an observer’s attention more readily. Even a blepharoplasty (if hidden entirely within the supratarsal crease) will fade away more quickly than an alar incision. Proper preoperative counseling will reduce potential postoperative headaches. The reader is reminded again that only a minority of patients (< 5%) qualify for all the criteria that justify alar-reduction surgery. Figure 9-1 (A-H) This 38-year-old Vietnamese man exhibits a wide, flat nasal configuration in which the alar width exceeds the nasal lobule, or tip, width. For this reason, he is a suitable candidate for alar-base reduction surgery. He also exhibits an overrotated and underprojected nasal tip and dorsum, which contribute to a feminized appearance to his nose. To attain a balanced look to his nose, he underwent concurrent alar-base reduction and augmentation rhinoplasty with a silicone implant. Figure 9-2 A nasal base that appears overly wide must be carefully evaluated to determine whether the nasal lobule or the nasal alae are responsible for this appearance. Alar reduction for a patient with a wide nasal lobule and narrow alae will only make the lobule appear even wider. Augmentation rhinoplasty of a wide nasal lobule with a silicone implant will impart the illusion that the nose appears narrower. Figure 9-3 A patient who exhibits flared nasal alae will benefit from alar-base reduction, and the nose can be made to appear even narrower with augmentation rhinoplasty of the nasal lobule using a silicone implant. Many types of alar-base excisions have been advocated in the literature3–5 (Fig. 9-6). The extent of soft-tissue excision and the shape of the wedge to be excised are dependent upon the amount of reduction that is desired. Furthermore, narrowing is partly accomplished by a cinching suture, as will be elaborated. When designing the wedge excision, the surgeon should consider the thickness of the ala and the risk of unnatural notching along the nasal sill. Accordingly, crossing the nasal sill should be undertaken with caution, experience, and judgment. The reader is referred to Sheen and Sheen’s textbook for a lucid discussion of this matter.6 Figure 9-4 Nasal width should always be viewed in the context of other facial features. A very wide face may not tolerate the appearance of a narrow nose. (A) The nasal length (from glabella to nasal tip, or subnasale) should occupy approximately one-third of the total vertical height of the face. The upper one-third of the face should extend from the hairline (trichion) to the glabella, and the lower one-third should cover the distance from the bottom of the nose to the lower aspect of the chin, or menton. (B): Horizontally, the nasal width should equal that of the eye, forming one-fifth of the total distance across the face. The distance from the lateral canthus to the lateral aspect of the ear should occupy the remaining fifth of the face. (From Williams EF, Lam SM. Comprehensive Facial Rejuvenation: A Practical and Systematic Guide to Surgical Management of the Aging Face. Philadelphia: Lippincott, Williams & Wilkins; 2004; with permission.)
Special Topics in Asian Rhinoplasty
♦ General and Anatomic Considerations
♦ Alar-Base Reduction
Preoperative Remarks



Surgical Technique

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


