Fig. 1
51-year-old patient with pigmentary changes and severe photoaging. (a, b) Pre-phenol peeling with occluded Baker’s formula. (c, d) Eight months after the peeling. Lifting effect and improvement of spots and wrinkles

Fig. 2
61-year-old patient. (a) Pre-peeling. (b) After Baker’s peel, with occlusion on perioral area
Due to its toxicity, phenol should be carefully applied, following the recommended technique and the contraindications. Patients should be monitored for emergency assistance in case of any systemic effect.
For this outstanding method of rejuvenation, there are numerous formulas; in this chapter, we will focus on deep chemical peeling with Baker’s formula (Table 1).
Table 1
Baker-Gordon formula
Component | Quantity |
|---|---|
Phenol USP 88% | 3 ml |
Distilled water | 2 ml |
Liquid soap | 8 drops |
Croton oil | 3 drops |
History
Phenol peeling and its secret formulas were held by aestheticians up to the early 1960s. Lay peelers are reported to be using formulas with phenol and croton oil in Hollywood since the early 1920s. They were famous for helping celebrities to keep their careers, and they proclaimed the technique as “the fountain of youth” (Hetter 2000a). A medical article dated 1917, by Montgomery, described an aesthetician that used occlusive phenol in New York (Hetter 2000a).
Over time, physicians would pay or permute information on these formulas, and in 1927, a surgeon from Los Angeles – H. O. Bames – described in details the occluded phenol peeling technique. He wrote about the importance of applying it by areas and with time interval between areas during procedure, which was not performed by most aestheticians. He also reported that they did not do it on the neck (Bames 1927). In 1959, Adolph Brown, from Los Angeles, patented a formula with phenol and croton oil (Hetter 2000b). In 1960, he published in the British Journal of Plastic Surgery the first detailed study of phenol formulas, histology, and toxicity after Bames’ study (Brown et al. 1960). In that paper, he outlined some of the incorrect dogmas that persisted for many years, such as (1) phenol is the active ingredient, (2) phenol penetrates more at lower concentrations, and (3) the addition of an agent that reduces the superficial tension increases penetration (Hetter 2000b, c). An example of an agent that reduces the superficial tension is Septisol® (liquid soap). Still in 1959, the plastic surgeon Clyde Litton obtained a formula from an aesthetician and presented, in 1961, in the Plastic Surgery Annual Meeting in New Orleans, the 2-year follow-up of 50 patients (Hetter 2000a, b). But the modern era of phenol peeling began when Thomas Baker obtained data from formulas held by three aestheticians and developed a modified solution of phenol with croton oil, Septisol®, and water (Table 1) and published it in 1962 in Plastic and Reconstructive Surgery (Baker 1962).
Although this formula is extremely strong, it has been the most commonly used and studied during all these years, probably because it is simple and it was the first formula fully published in a journal of great circulation among plastic surgeons.
After that, among numerous papers, those by Stegman in 1980 and 1982 (Stegman 1980, 1982) brought a more controlled and scientific understanding of peelings. He concluded that some factors may enhance the skin injury of Baker’s formula: 1) increase in phenol concentration; 2) greater number of layers of Baker’s emulsion; 3) and occlusion, offering greater penetration. Also, by removing croton oil, less injury was obtained from Baker’s formula. In 1996, histological studies by Moy et al. (1996) reinforced Stegman’s findings, stating that the more intense and deeper reaction of Baker’s peeling is due to the combination of the ingredients.
The series of articles by Hetter in 2000 (2000a, b, c, d) reported a relevant role of croton oil in phenol peeling. Varying its concentration a proportional modulation of the peeling’s penetration is obtained. Phenol concentrations were also studied. A more intense tissue reaction was observed with higher concentrations of phenol, therefore challenging Brown’s dogmas. The surfactant’s (soap or detergent) role is to decrease the superficial tension, emulsifying more easily the oil and phenol/water mixture, allowing a more even application.
Phenol-Croton Oil Peeling: Toxicity
Phenol
Phenol – or carbolic acid – consists of a benzene ring with a hydroxyl group, derived from coal tar or synthesized from monochlorobenzene. It is bacteriostatic at 0.2%, is bactericide at concentrations higher than 1%, and has an anesthetic effect at 5%.
Phenol is rapidly absorbed percutaneously; 70% of phenol applied to the skin is absorbed within 30 min (Wexler et al. 1984). The absorbed phenol is eliminated through three processes: excretion, oxidation, and conjugation. After absorption, 25% is metabolized into carbon dioxide and water. The remaining 75% may be excreted unchanged through the kidneys or conjugated with glycuronic or sulfuric acids. A small quantity may also be oxidized into hydroquinone and pyrocatechin. Both oxidation and conjugation occur in the liver (Litton 1962).
Signs of systemic toxicity include nausea, vomiting, paresthesia, headache, and obnubilation. Central nervous system stimulation may manifest initially with tremors, hyperreflexia, and hypertension and then followed by central nervous system depression. Poisoning, due to accidental ingestion, causes sudden nervous system depression, cardiorespiratory arrest, and hepatorenal failure.
A phenolemia of 0.68 mg/dl was obtained 1 h after a 3 ml of 50% phenol application all over the face. This represents a safety margin against 23 mg/dl dosed 15 min after phenol ingestion (Litton 1962). Unfortunately there isn’t a reliable estimate of the lethal dose due to the great variation of phenol levels in the blood after exposure.
In peelings, phenol absorption and toxicity seem to be more dependent of the total skin area exposed at once than merely the concentration of the agent. Systemic toxicity, if occurs, starts a few minutes after application, but no hepatorenal or central nervous system problems have been reported with phenol peeling when appropriately performed.
However, cardiac arrhythmias have been associated with this peeling rapidly applied all over the face (Truppman 1979), once phenol is directly toxic to the myocardium (Stagnone et al. 1987). Another rationale for cardiotoxicity is the release of adrenaline due to the pain, transmitted from the trigeminal nerve to the cardiac vagus nerve or from the cerebral cortex directly to the sinoatrial node (Stagnone and Stagnone 1982). The application at each cosmetic unit followed by a pause seems to reduce the risk of cardiac toxicity .
Diuresis promotes the excretion of phenol and reduces arrhythmias. The alkalinization of urine may also contribute by increasing the renal tubular excretion (Matarasso 1994).
If a mild supraventricular arrhythmia occurs, application should be discontinued until the sinus rhythm returns to normal. It is advisable to wait 15 min after the normalization of the rhythm before resuming the procedure. If a severe supraventricular or a ventricular arrhythmia occurs, phenol should be replaced with another exfoliating agent (Brody 1997a).
It is useful to understand that the efficacy of a chemical agent can be modified by associations with other agents that modulate its potency and toxicity.
It is tried to “tame” phenol, as well as trichloroacetic acid, by associating them with additives, emulsifiers, saponins, and surfactants that increase the efficacy and safety of these exfoliating agents. Thus, for example, knowing that the low molecular weight of phenol (94,11) and its polarity allow it to rapidly pass through the cell and endothelial membranes and that it is more rapidly absorbed in an aqueous solution than in an oily solution; it is found in many modified formulations, glycerin, sesame, and/or olive oils, which solubilize phenol and reduce its systemic absorption and aggressiveness (Deprez 1998).
Croton Oil
Croton oil is extracted from the seed of Croton tiglium, a native shrub from India and Ceylon. It is composed of 7% glycerin, 37% oleic acid, 19% linoleic acid, 7.5% myristic acid, 1.5% arachidic acid, and less than 1% stearic, palmitic, lauric, valeric, tiglic, butyric, acetic, and formic acids. Croton oil was used as a purgative in India and introduced in Europe in 1630 for that purpose, and it may even lead to death. On the skin, it may cause vesiculation, necrosis, and severe burning (Hetter 2000c).
Deep Peeling Modalities
Occlusion
Deep peeling may be occluded or not (Figs. 3, 4, and 5). Occlusion acts as a mechanic barrier against phenol evaporation and increases skin maceration, promoting higher absorption and deeper penetration. Occlusion may be performed using strips of impermeable adhesive tape, measuring 1–1.5 cm wide, overlapped in two to three layers, and placed directly on the skin for 48 hours (Figs. 6 and 7). However, patients feel a little discomfortable, and many will prefer occlusion with petrolatum (Stuzin 1989) or silicone gel, immediately applied on the phenol-treated skin. But be aware that phenol may be carried together with the petrolatum or silicone gel into the eyes due to the capillarity through the wrinkles. So in our practice, we do not recommend the application of petrolatum or silicone nearby the eyelids during or just after the procedure.





Fig. 3
(a) 56-year-old patient, pre-phenol peeling with non-occluded Baker’s formula. (b) Immediately after, showing edema and erythema on face
Fig. 4
The same patient of Fig. 3. (a) 24 hours post-peeling. Severe edema and darker coloration of the face. (b) 48 h post-peeling, before washing the face. Edema, fibrin, skin scaling and detachment. (c) 48 h post-peeling. Cleaner face after removal of secretion, fibrins and detached skin
Fig. 5
The same patient of Figs. 3 and 4. (a) 4 days post-peeling, using petrolatum ointment, already without necrotic epithelium, but with diffuse erythema and some fibrin areas. (b) 12 days post-peeling, skin reepithelized, but still with erythema. (c) 2 months post-peeling showing improvement of flaccidity and wrinkles
Fig. 6
67-year-old patient. (a) Pre-phenol peeling with occluded Baker’s formula. (b) Immediately after the adhesive tape mask. Note the eyelid edema initiating and the use of a compression dressing (not routinely used). (c) 24 h post-peeling with more eyelid edema
Fig. 7
The same patient of Fig. 6. (a) 48 hours post-peeling, before adhesive tape removal. Improvement of eyelid edema. (b) 48 hours post-peeling. Adhesive plaster removal. Note the epithelium adhered to the adhesive tape, humid skin with secretion, fibrin, and necrotic epithelium. (c) 3 days post-peeling, face with erythema and edema, scale, and fibrin
Among the various post-peeling occlusion techniques, thymol iodide powder or bismuth subgallate powder may be used after the removal of the adhesive plaster. They form a second mask that stays in place for 6–9 days (Figs. 8, 9, and 10). This mask is reported to avoid mobilization and to improve wound healing which results in a more even peeling. With this second mask, wound care is not needed, with the benefit that the skin will be fully reepithelized after mask removal. Patient support is advisable, since they may feel a little depressed with the use of this mask for several days.



Fig. 8
The same patient of Figs. 6 and 7. (a) 6 days post-peeling, face more reepithelized with erythema, dry skin, and scaling. (b) 10 days post-peeling, face reepithelized with erythema, edema, and dry skin. (c) 15 days post-peeling. Note the irregularity of application on the left side of the eyelid and lip border
Fig. 9
4 days with bismuth subgallate powder mask
Fig. 10
7 days with bismuth subgallate powder mask, removed with small amount of petrolatum
Baker’s Formula
The old Baker’s formula, published in 1962, is still up-to-date and is the most commonly used (Table 1).
Baker-Gordon’s formula is prepared by drawing up 3 ml of phenol into a syringe and depositing it into a recipient. Next, 2 ml of water, eight drops of liquid soap, and finally, three drops of croton oil are added. This dilutes the concentration of phenol to about 50%. It is an immiscible emulsion and should be well stirred at each application (Figs. 11, 12, and 13). Hetter (2000c) shows that peelings with increasing concentrations of phenol at 18%, 35%, and 50% with Septisol® soap and without croton oil, respectively, cause an increased reaction of edema and erythema without significant dermal injury, while 88% phenol without Septisol® causes injury to the dermis. The addition of croton oil to 50% phenol, however, causes remarkable increase of peeling depth in the dermis.
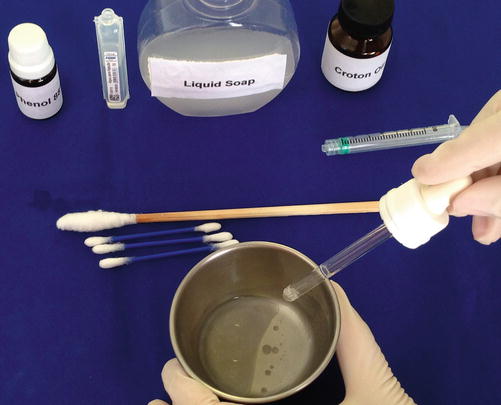

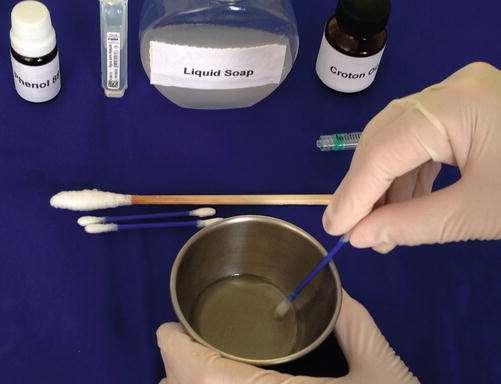
Fig. 11
Baker’s formula preparation. Immiscible emulsion
Fig. 12
The addition of croton oil with syringe, considering 1 drop as equivalent to 0.04 ml. Note, the croton oil measured with a dropper may vary due to the dropper size
Fig. 13
Homogenized emulsion after well stirring
The same author (Hetter) reports in a personal communication that 33% phenol may produce a mild medium-depth, deep medium-depth, or deep peeling when the croton oil concentration varies of 0.35%, 0.7%, or 1.1%, respectively (Stone 1998). Hetter associated with a 16–50% phenol solution associated with croton oil between 0.25% to 2.78% used healing time to judge peeling depth and concluded that peel depth increases with the concentration of both agents (Hetter 2000d). Croton oil concentration in Baker’s formula is 2.08% and seems to play an important role on the peeling depth.
Other studies seem to confirm histologically Hetter’s statements about the role of phenol and croton oil concentration (Moy et al. 1996; Stone 1998). Nevertheless other factors may influence depth such as occlusion method, pressure exerted in the application, friction, the number of coats on the same area, exposure time to the substance, volume applied, vehicle used, and patient skin type. When using Baker’s formula, which is quite concentrated, it is important to take these into account so that occlusion is not always necessary to achieve the desired results.
There are numerous other formulas before and after Baker’s; however, some of them were or still are secret in their entire composition, and currently there are some commercial products for sale.
Phenol “Neutralizers”
Phenol is soluble in oil and can be rapidly removed from the skin with glycerin, propylene glycol, vegetal oils, or 50% alcohol.
However, topically, phenol in high concentrations causes an extremely quick denaturation and coagulation of keratin (frosting), which is irreversible.
Indications
Phenol peeling is indicated for rejuvenation of skins with more severe, thin, and mosaic wrinkles in order to correct pigmentary changes, actinic damage, and irradiated skin damage if the adnexa are present for reepithelization (Figs. 14, 15, and 16).



Fig. 14
Pre-phenol peeling, thin wrinkles in a mosaic pattern. (a) Frontal view. (b) Right frontal-lateral view
Fig. 15
The same patient of Fig. 14, 4 months post-phenol peeling. (a) Frontal view. (b) Right frontal-lateral view
Fig. 16
(a) Pre-phenol peeling, Skin presenting photoaging, pigmentary changes, and flaccidity. (b) 3 months post-phenol peeling
Traditionally, it is indicated for patients with Fitzpatrick skin types I to III, once phenol – as well as other deep exfoliation procedures – may cause hypopigmentation . Light skins also have lower possibility of visible contrast between the treated and untreated skin. However, localized peelings in types I and II patients may produce contrast between the thicker, elastotic, yellowish photodamaged skin and the treated thinner rejuvenated area without spots. When this occurs, the only option is to treat the entire face (Stuzin 1998). Some authors also state that, in types I and II with naturally less pigment, the hypochromia, even when uniform all over the face, may sometimes draw more attention than in types III and IV. In the latter patients, hyperpigmentation is the rule but often reversible. It is not advisable to perform a deep phenol peel in skin types V and VI, due to the high risk of post-inflammatory hyperpigmentation, irregular hypopigmentation with vitiligo-like appearance, and keloid.
Contraindications
Contraindications to phenol peeling include cardiac, renal, or hepatic diseases and skin phototypes V and VI.
Relative contraindications include herpes simplex infection, hormone therapy with estrogen or progesterone, continuous or prolonged exposure to ultraviolet light that may lead to post-peeling hyperpigmentation, recent use of isotretinoin that may lead to healing changes, psychological problems or unrealistic expectations, previous ionizing radiation therapy, skin phototypes III and IV, predisposition to keloids , anatomic location with few adnexa, and recent facial surgery with undermining or flaps .
Pre-peeling Preparation
Prior to procedure, one should:
Obtain the patient’s consent providing treatment options and information about the technique, discomfort, dressings, time to heal, complications, and long-term care with emphasis on photoprotection.
Obtain the patient’s clinical history with special attention to cardiac, renal, and hepatic diseases.
Request the patient’s previous electrocardiogram, complete blood count, and biochemistry, including kidney and hepatic function.
Take photos of the patient before the peeling.
Unlike other peelings, previous preparation of the skin is not mandatory. In case there was previous use of topical agents, such as retinoid and other acids, check if there is no skin irritation that could lead to an undue peel deepening.
Prophylaxis for herpes simplex infection is mandatory, with or without previous history. Acyclovir 400 mg three times daily, valacyclovir 500 mg twice daily, or famciclovir 250 mg twice daily is recommended, initiated 1 or 2 days prior to the procedure and maintaining it for 10–14 days. Note that cases of herpes infection may occur even after full reepithelization (Perkins and Sklarew 1996).
Bacterial and mycotic infections are rare and, in general, do not require prophylaxis on phenol peeling.
Technique (Full-Face Phenol Peel)
General Care and Safety
Phenol peelings should be performed with supportive equipment and staff, cardiac monitoring, and potent analgesia, preferably in a hospital for greater patient and medical staff safety. Use a ventilated room (to dissipate phenol) and always have cardiopulmonary resuscitation (CPR) equipment and emergency medications available and easily accessible. The patient should be fasting, with an intravenous access, cardiac monitoring, and pulse oximeter installed (Fig. 17).

Fig. 17
Patient monitored and with intravenous access
Local Care and Edge Delimitation of the Peeling
Instruct the patient to perform facial hygiene, usually in the morning of the procedure, and to avoid the use of makeups (Brody 1997a).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


