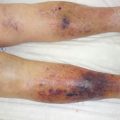
Fig. 16.1
(a) The picture shows two fang marks on the left ring finger. Swelling and tissue necrosis are visible around the fang marks. (b) The picture shows that the left knee was swollen with an area of soft tissue necrosis measuring 3.5 × 2.0 cm around the fang marks. (c) Histopathological findings of the fang mark site immediately after injury. The image shows red cell extravasation, vessel fibrinoid necrosis, and subcutaneous hemorrhagic necrosis with neutrophil infiltration
16.3 Dry Bite
The severity of a snakebite depends on the size of the snake and severity of envenomation. Venomous snakes sometimes bite without injecting venom. Such “dry bites” are known to occur in a number of venomous snake species and may account for in excess of 50 % of “accidental” bites in some species. The quantity of venom can vary depending on the size of the snake, and the venom contents also vary at the time of the bite [8].
16.4 First Aid
“Guidelines for the Management of Snake-Bites” by the World Health Organization (2010) [10] recommends the following: the victim must avoid physical activity, and the bite site should be immobilized and kept below heart level to prevent venom absorption and systemic spread. Tourniquet application, incision, excision, or mouth suction should not be performed. Many organizations, including the American Medical Association and American Red Cross, recommend washing the bite with soap and water. The use of a compression bandage is generally as effective; however, some guideline states that nonprofessionals should not apply a pressure bandage (Fig. 16.2) [1].

Fig. 16.2
Pressure immobilization using a compression bandage
16.5 Antivenom Treatment
Antivenom is still the only effective treatment for envenomation. It is indicated to reduce convalescence time in moderate to severe cases and prevent death in severe cases. The British National Formulary suggested that antivenom should be given whenever there is any evidence of systemic envenoming or when local symptoms of envenoming are severe if, within 4 h of a bite on the hand or foot, swelling extends beyond the wrist or ankle [8]. There is evidence that antivenoms limit the spread of necrosis by inhibiting protease activity and reducing edema, leading to decreased risk of compartment syndrome.
16.6 Allergic Reactions to Antivenom
Allergic reactions to antivenom are possible. The most common reaction to antivenom is an anaphylactoid reaction, in 3–54 % of patients. Ismail et al. reported that 40 % of patients showing early reactions develop systemic anaphylaxis.
Serum sickness-type reactions have been reported to occur in 10–75 % of patients receiving equine antivenin. The onset of delayed serum sickness usually occurs within 3 weeks after antivenin treatment and consists of fatigue, itching, urticaria, arthralgia, lymphadenopathy, periarticular swelling, albuminuria, and, rarely, encephalopathy [6].
Patients who have had prior reactions to horse serum and those who have had previous antivenin treatments can develop severe, delayed hypersensitivity reactions.
16.7 Surgical Treatment
Most of the literature is focused on snakebite mortality. However, many patients survive and suffer from local complications. Although snakebites are most commonly treated with specific antivenoms, surgical management has also been practiced. A meta-analysis reported an incidence of 5.5 % sequelae and 3 % amputations. Snakebite patients with skin necrosis require serial wound debridement, followed by reconstructive surgery using skin grafting and/or a flap. Chattopadhyay et al. reported that 28 % of 58 patients required debridement to treat local necrosis. Maintenance of necrotic tissue in the wounds will certainly aggravate the local and general conditions of patients [2]. Surgery plays an important role in the management of snakebite patients with tissue necrosis. However, this involves late debridement, performed after skin necrosis has occurred.
16.8 Immediate Debridement of Fang Marks
If a snakebite is intracutaneous, the venom slowly spreads through lymphatic and superficial venous vessels, but there has to be a sufficient venom concentration to reach the systemic circulation in a few hours.
Recent guidelines for first aid against viper envenomation call for avoiding incision and recommend the administration of antivenom. However, antivenom carries the risk of an anaphylactic reaction, so its usage should be approached with extreme caution.
Since the snakebite severity depends on the amount of venom injected into the victim, if even a small part of it can be removed, patients should present milder symptoms.
Even in the case of perfectly performed incision and suction, only 20 % of venom can be removed. Also, since snake fangs are curved, the venom is not directly under the bite marks; therefore, only a very deep incision can reach it [1]. To prevent later sequela, snakebites are best treated acutely by surgical debridement to remove as much venom as possible, which consequently decreases inflammatory responses and the necessity of antivenom [7].
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


