Chapter 19 Secondary Rhinoplasty
 Animations
AnimationsPearls
• In communicating with secondary rhinoplasty patients, any statement or gesture of disapproval of what was done during the previous surgery should be avoided.
• Patients who have telangiectasis as a result of the initial surgery may experience deterioration of this condition after the secondary surgery.
• The telangiectasis can be eliminated with vascular laser (wavelength 585 nm).
• For patients with thin skin, one has to be prepared to use fascia, dermis, or perichondrium to augment the soft tissues.
• The inverted V deformity is not usually discernible intraoperatively or for some time after the surgery, often taking 6 months and up to one year or longer to become noticeable.
• Over-resection of the supratip structures, which may cause a dead space filled with blood and formation of fibrofatty tissues, or under-resection of the caudal dorsum followed by loss of tip projection, can result in formation of supratip (Polly beak) deformity.
• Dome division techniques without additional measures can result in too much narrowing of the tip, bossae formation, asymmetry, migration of the medial crura and medial genu caudally over a long period of time, and loss of projection due to loss of stability of the tip triad.
• Patients who seem to have unrealistic expectations, demand perfection, or make disparaging remarks about the previous surgeon may not be suitable candidates for a secondary rhinoplasty.
• Due to scar tissue, dissection through an open technique following a previous exonasal surgery is far more time-consuming than this operation after a previous endonasal approach.
• Overcorrection of the radix deficiency can be significantly more detrimental to the facial balance than the deficiency itself and may make the eyes appear too close to each other, which in most cases is undesirable.
• Revision surgery for a large residual dorsal hump may require osteotomy to narrow the distance between the nasal bones and also the use of spreader grafts.
• A cephalocaudal groove over the mid-portion of the nasal bone due to an anterior position of the osteotomy can be corrected with a second osteotomy in a low-to-low level.
• For a larger dorsal defect, a septal or conchal cartilage graft has to be used, although this goal can also be accomplished using diced cartilage graft. A smaller dorsal defect can be eliminated using a piece of conchal cartilage graft.
• For patients who have significantly attenuated lower lateral cartilages with major collapse of the internal valve, a splay graft would be best.
• For an isolated inverted V deformity without dorsal profile deficiency, bilateral spreader grafts can be inserted through a small incision approximately 3 mm long and placed anteroposteriorly along the caudal border of the lower lateral cartilages.
• For secondary rhinoplasty patients with a deficient lobule volume, either an onlay or a shield graft can be used if infratip lobule volume augmentation is also necessary.
• While a differential level of 6–10 mm between the domes and the dorsum is necessary on primary rhinoplasty patients, this reduces to 3–4 mm on most secondary patients, especially if the tip skin is thin.
• A nostril can be elongated on a secondary rhinoplasty patient by using a combination of a columella strut, approximation of the footplates, removal of a crescent piece of soft triangle lining and application of an alar rim graft.
• Presence of a significant amount of scar tissue may limit the success of secondary rhinoplasty.
• To repair a chronic perforation of the septum through a small transfixion incision, a pocket is created involving the perforation site and extending beyond the margins. A straight piece of septal cartilage or a perpendicular plate of the ethmoid bone or PDS plate is placed in position, and extramucosal splints are applied to both sides, to avoid free flow of air, and kept in position for at least two weeks.
• Many secondary rhinoplasty patients who have had a partial turbinectomy involving either the anterior or posterior portion of the turbinate will have a compensatory enlargement of the intact portion of the turbinate.
Dealing with the secondary rhinoplasty patient is totally different from attending to a patient who is undergoing a primary rhinoplasty. A secondary rhinoplasty presents additional emotional, physical, and anatomical challenges.1–5 A positive outcome requires a clear understanding of patient concerns, precise definition of nasal flaws, and establishment of achievable goals. Thorough knowledge of the nuances and potential problems as well as additional prudence during the surgery are necessary to deliver a satisfactory outcome. In this chapter, the author will discuss the elements that set a secondary rhinoplasty apart from a primary rhinoplasty, the many nuances that govern the management of secondary rhinoplasty patients, patient assessment, surgical planning, technical details, and graft sources.
Patient Evaluation
A patient seeking a primary rhinoplasty may not be cognizant of any functional difficulties, while a secondary rhinoplasty patient is often clearly aware of the limitations in breathing commonly associated with flaws in the form of the nose. While the former group has no base with which to compare current breathing capacity, the latter group is able to compare current breathing with their breathing before the primary rhinoplasty. Therefore, such patients are keenly aware of the reduced functional capacity of the nose. A deterioration in breathing is often the result of valve dysfunction caused by malposition of the upper lateral cartilages, nasal osteotomy, and medial repositioning of the nasal bone, which can often dislodge the inferior turbinates and the upper lateral cartilage, or of external valve dysfunction.6–8 However, some airway deterioration is related to the failure of the previous surgeon to recognize underlying breathing problems and marginal airflow that were easily disturbed by even minor anatomical changes.
Physical Assessment of the Nose
It is important to determine, through a careful examination, whether a septoplasty and turbinectomy has been performed. Any surgical steps recorded in the operative notes available from the previous surgery should be substantiated by the examiner. There is a tremendous variation in the magnitude of septoplasty and this can only be ascertained by a thorough examination. The forceful opinions and statements of secondary rhinoplasty patients about their noses can be a source of distraction, wrongly causing the surgeons they visit to focus attention directly on the nose rather than on the entire face. It is therefore imperative to examine the complete face before centering the attention on the nose. Any imperfections marring the forehead, such as prominence or retrusion; chin abnormalities, including macrogenia, microgenia, or asymmetry;9–10 underdevelopment of the malar bones; and maxillary and mandibular disharmony should be noted. Sometimes, these factors are substantial sources of incongruity. For example, a severely receding chin may make the nose appear overprojected when in reality the problem is the chin deficiency. Should disharmonies of the face related to the other structures go undetected, the outcome of the secondary surgery, like the primary surgery, will still be disappointing. The flawed features should be brought to the patient’s attention and corrected, if the patient is in agreement. Insistence on correcting these additional imperfections of the face as a condition of proceeding with the rhinoplasty should be avoided. However, it is crucial to inform the patient of the consequences of not correcting other flaws that indirectly will influence the rhinoplasty outcome.
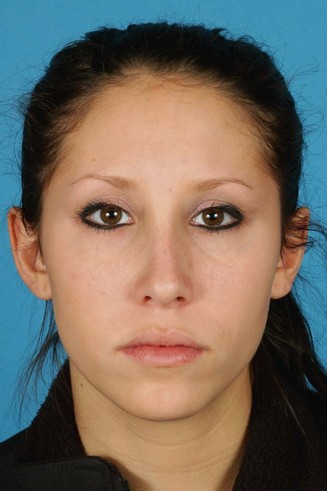
As in assessment of a primary rhinoplasty patient, the external nose examination begins with observation of the thickness of the skin. If the patient has thick, sebaceous nose skin (Figure 19.1), it is likely that, at least to some degree, the previous surgery failed because of this unfavorable condition. If skin thickness was a major factor, subsequent surgery may not produce a much improved outcome unless the condition of the skin is changed as much as feasible. This adverse condition should be discussed with the patient to reduce the patient’s expectations of surgery. Patients with heavily sebaceous skin are suboptimal candidates for an external incision, whether it is used for an open technique or in alar-based surgery. Referral to a dermatologist and a resolute effort to reduce the sebaceous and porous nature of the skin may prove helpful in these circumstances. Tretinoin or isotretinoin can be prescribed under the supervision of a dermatologist to lessen the activity of the sebaceous glands. However, surgery should then be delayed for at least 6 months to minimize the potential of excessive bleeding and formation of hypertrophic scars in those taking tretinoin. Additionally, the technique should be modified to achieve better tip definition for patients with thick skin in the tip area, creating a narrower tip frame. Furthermore any supratip dead space should be eliminated by approximation of the skin to the underlying frame. Otherwise blood can accumulate in this space and ultimately convert to fibrofatty tissue. This obscures the definition of the nose and often results in a supratip deformity (see Chapter 15).11

Figure 19.1 A secondary rhinoplasty candidate with significant sebaceous activity causing thickening of the skin.
Patients who have telangiectasis as a result of the initial surgery may experience deterioration of this condition after secondary surgery (Figure 19.2). Informing the patient of the potential for this will avoid dissatisfaction and prepare the patient for postoperative treatment with vascular laser (wave length 585 nm) to reduce or eliminate telangiectasis. Observation of suboptimal scars from previous surgery may predict similarly poor scars following secondary rhinoplasty. The patient should be forewarned of this possibility, if it is detected.

Some patients have thin skin (Figure 19.3), particularly over the dorsum of the nose, as a result of dissection in a plane superficial to the periosteum during the previous surgery, which ultimately results in removal of the periosteum along with the residual hump. This is why the importance of dissecting in the subperiosteal plane during primary surgery is stressed, to ensure that the periosteum is maintained to cover the underlying frame. Patients with thin skin should be informed that they may need one of a variety of soft tissue grafts, such as dermis, fascia, or perichondrium. When the skin is very thin, it may take on a red or purplish color, which often becomes a source of concern to the patient. This is particularly likely when dorsal augmentation has been achieved using alloplastic materials. The discoloration may be more obvious in a cold environment. When a soft tissue graft is added to the dorsum, the skin color may return to normal.

The Radix
After examination of the skin, the external nose is assessed in an organized fashion starting from the radix. A shallow radix, which produces a displeasing transition from the forehead to the dorsum, is extremely common. Failure to use the effective tools available to lower this site is the most common reason for failure to correct radix fullness (Figure 19.4). Another common finding is a radix that is too deep. Usually, this is a pre-existing condition that has not been corrected adequately. However, in some patients the radix may have been over-reduced.

The Bony Dorsum
Examination of the nasal bones may disclose some irregularities, a very common cause of concern for secondary rhinoplasty patients. Optimally, one would like to see two parallel dorsal lines extending from the eyebrows to the supratip area without any interruption. Frequently, these lines are interrupted because of imperfections in the nasal bones (Figure 19.5). When the nasal bone osteotomy is carried out low-to-high (too anteriorly), rather than low-to-low, a step created by the osteotomy may be seen midway between the dorsal line and the junction of the nose with the face (Figure 19.6). Other dorsal imperfections include a dorsum that is too narrow or too wide.

The Midvault
The midvault can also be marred by excess width or too much narrowing, creating an inverted V deformity (Figure 19.7). This is almost invariably the result of over-resection of the midvault and loss of support of the upper lateral cartilages, allowing them to shift medially and consequently narrowing the internal valve. Over-resection of the dorsum also results in depression in the midvault area. An increased awareness of this flaw and repeated recommendations at rhinoplasty educational courses to use spreader grafts have reduced the incidence of this deformity. The deformity is not usually discernible intraoperatively or for some time after surgery, often taking 6 months and occasionally up to 1 year to become noticeable. Rarely, in patients with very thick skin, it can take several years before the deformity is detectable. Some inverted V deformities are not noticeable even for decades, until the skin thins as a result of aging.

The Supratip Region
The role of the supratip break in the aesthetics of the nose has been underemphasized. Over-resection of the supratip structures, creating too much of a differential level between the domes and the anterocaudal septum, can result in exaggerated supratip definition, although this is not nearly as displeasing as supratip fullness causing a supratip or ‘Polly beak’ deformity. This deformity is sometimes a consequence of too much resection of the dorsum and failure to eliminate dead space, which can result in collection of blood and ultimately the formation of fibrofatty tissue,11 as mentioned above. However, it is not uncommon to have supratip fullness related to the residual anterocaudal dorsum (Figure 19.8), which may become further exaggerated by loss of tip projection during healing. In secondary rhinoplasty patients, detection and correction of this flaw constitutes a principal step without which neither the patient nor the surgeon will be pleased.

The Nasal Base
The nasolabial angle is another aesthetic feature that plays an enormous role in the congruity of the nose. Cephalic over-rotation of the tip, causing an obtuse angle, is a hallmark of rhinoplasties performed in the 1970s and early 1980s. Ironically, a large number of secondary rhinoplasty patients today have a narrow nasolabial angle and are dissatisfied because the tip is not adequately rotated cephalically. Furthermore, the columella may appear too caudal (Figure 19.9) or too cephalad in relation to the rim. There are patients who have hanging ala, giving the appearance of a retracted columella even though the flaw does not actually involve the columella. Similarly, patients may have a retracted alar rim, which is extremely common (Figure 19.10), and makes the columella look as if it is protruding excessively. The alar base can be asymmetric, too wide, or, rarely, too narrow. The alar base can also be either cephalically or caudally malpositioned.


A basilar view may demonstrate misshapen nostrils, dome malposition, asymmetry, excessive infratip lobule volume with short nostrils, or nostrils that are too long with sufficient lobule volume, causing an imbalance of the basilar unit (Figure 19.11). In this view, one commonly sees a deviation of the columella, footplate malposition, and alar base asymmetry.

Nasal valve function should be assessed by asking the patient to inhale forcefully (Figure 19.12). This will reveal any collapse of the internal or external valves. Examination of the nasal valve using a speculum or a Q-tip can provide additional information and confirm nasal valve dysfunction seen on external observation. Such patients should also be examined carefully to assess the amount of residual septal cartilage, presence, location and size of a potential septal perforation, enlarged turbinates, and the presence of synechiae, polyps, or other abnormalities that could be causing airway compromise. The septum should also be carefully examined for residual deviation, which is extremely common.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


