Chapter 15 Rotational and Free Flap Closure of the Abdominal Wall 
1 Preoperative Considerations
1 Comorbidities
 Skin and subcutaneous fat may be of varying thicknesses and qualities in patients because of body habitus, scarring, steroid use, malnutrition, advanced age, and other factors.
Skin and subcutaneous fat may be of varying thicknesses and qualities in patients because of body habitus, scarring, steroid use, malnutrition, advanced age, and other factors.







3 Timing
 Optimize the patient before closure of the abdominal wall in regard to nutrition, cardiovascular status, and pulmonary function. The closure may lead to prolonged intubation, and this risk is increased in patients with chronic obstructive pulmonary disease (COPD) and smokers.
Optimize the patient before closure of the abdominal wall in regard to nutrition, cardiovascular status, and pulmonary function. The closure may lead to prolonged intubation, and this risk is increased in patients with chronic obstructive pulmonary disease (COPD) and smokers.







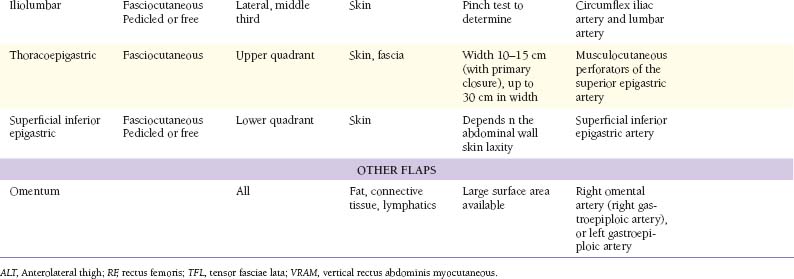
2 Muscular Flaps (Table 15-1)
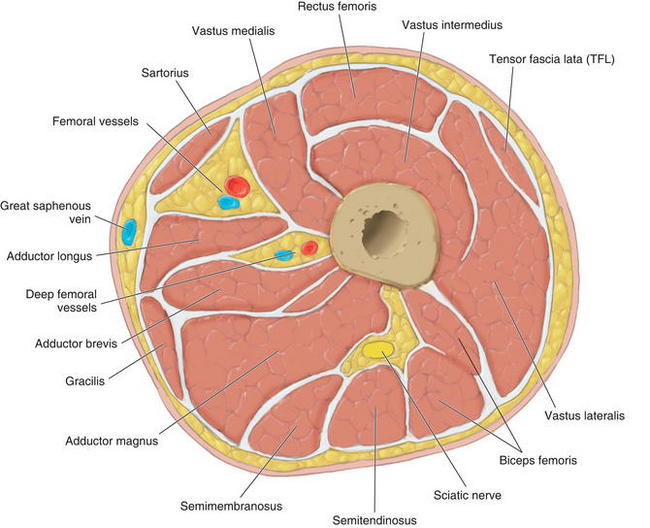
 Figure 15-1 shows the cross-sectional anatomy of the thigh demonstrating the possible muscles for coverage of abdominal wall defects
Figure 15-1 shows the cross-sectional anatomy of the thigh demonstrating the possible muscles for coverage of abdominal wall defects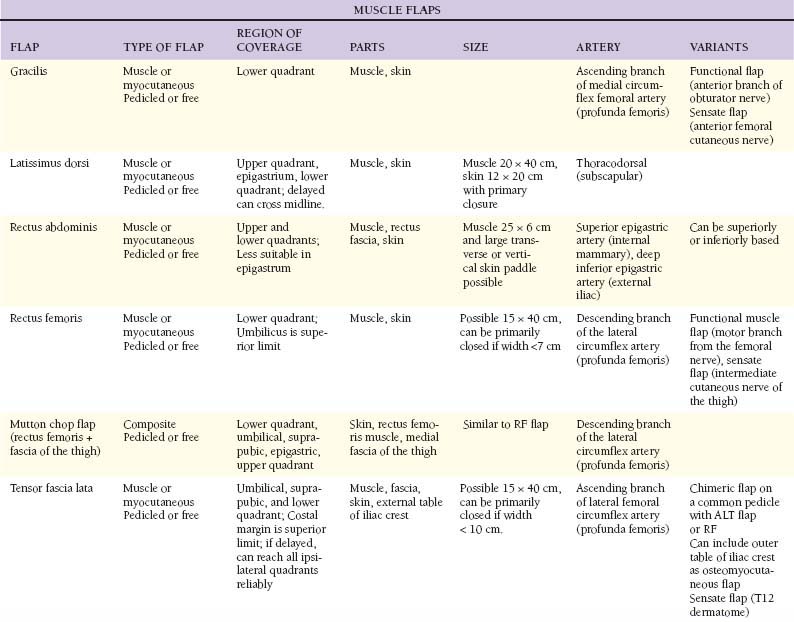

1 Tensor fascia lata
 Anatomy
Anatomy




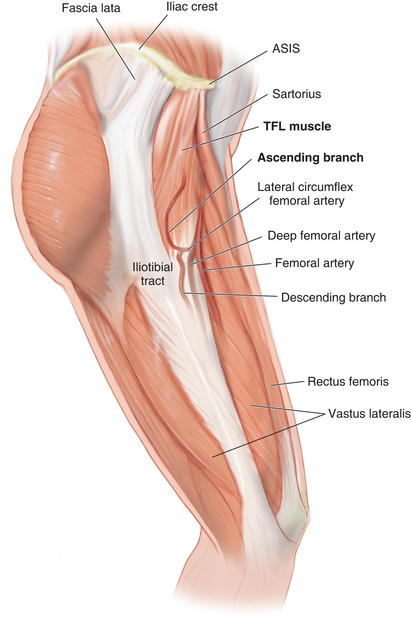
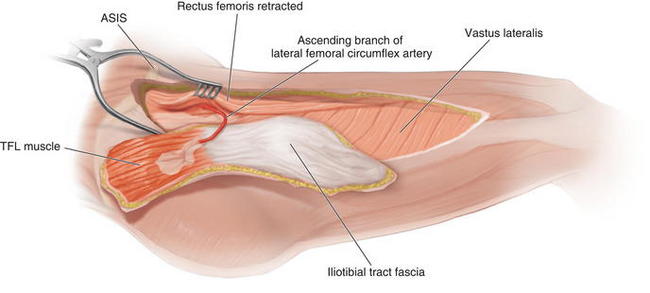
 The descending branch of the lateral femoral circumflex artery continues beyond the TFL muscle to supply the skin of the anterolateral midthigh and the lower thigh. It can be harvested with the anterolateral thigh skin to enlarge the perfused vascular territory.
The descending branch of the lateral femoral circumflex artery continues beyond the TFL muscle to supply the skin of the anterolateral midthigh and the lower thigh. It can be harvested with the anterolateral thigh skin to enlarge the perfused vascular territory. The TFL muscle (Fig. 15-2) is a short, flat muscle that is approximately 12 to 15 cm long. It acts as an accessory flexor and medial rotator of the thigh. It originates from the anterior iliac crest and the deep surface of the fascia lata. At the origin, it lies between the gluteus medius and sartorius, and superficial to the vastus lateralis. It inserts into the iliotibial tract, which inserts distally on Gerdy’s tubercle on the lateral aspect of the tibia.
The TFL muscle (Fig. 15-2) is a short, flat muscle that is approximately 12 to 15 cm long. It acts as an accessory flexor and medial rotator of the thigh. It originates from the anterior iliac crest and the deep surface of the fascia lata. At the origin, it lies between the gluteus medius and sartorius, and superficial to the vastus lateralis. It inserts into the iliotibial tract, which inserts distally on Gerdy’s tubercle on the lateral aspect of the tibia.
 Flap Design
Flap Design
 Skin territory can be up to 15 × 40 cm. A line from the ASIS 10 to 15 cm posteriorly marks the origin of the TFL muscle, with the skin territory extending 2 cm cranial to this line (Fig. 15-3). The lower skin territory is 8 cm above the lateral femoral condyle. Posterior skin territory is a line drawn from the greater trochanter to the fibular head or approximately along the axis of the femur. The anterior border is a line drawn from the ASIS to the lateral aspect of the patella.
Skin territory can be up to 15 × 40 cm. A line from the ASIS 10 to 15 cm posteriorly marks the origin of the TFL muscle, with the skin territory extending 2 cm cranial to this line (Fig. 15-3). The lower skin territory is 8 cm above the lateral femoral condyle. Posterior skin territory is a line drawn from the greater trochanter to the fibular head or approximately along the axis of the femur. The anterior border is a line drawn from the ASIS to the lateral aspect of the patella.
 The rotation arc of the pedicled flap reaches the costal margin if the tensor muscle is completely detached from its origin and raised as an island flap.
The rotation arc of the pedicled flap reaches the costal margin if the tensor muscle is completely detached from its origin and raised as an island flap.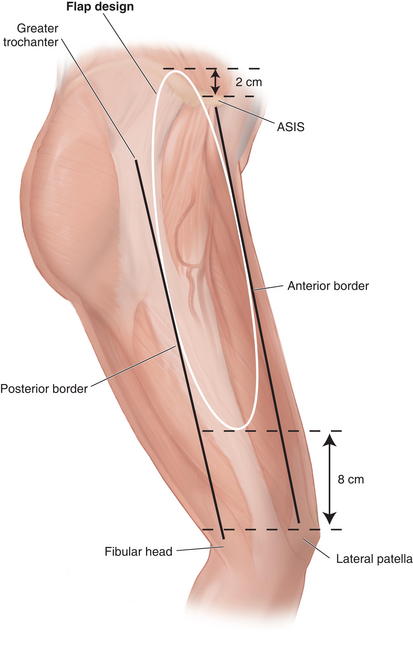
 Marking and Dissection
Marking and Dissection
 The flap is marked as an ellipse over the axis of the TFL muscle and to incorporate the pedicle proximally.
The flap is marked as an ellipse over the axis of the TFL muscle and to incorporate the pedicle proximally.












 Postoperative Care
Postoperative Care
 The donor site can be closed primarily if planned appropriately. Skin graft may be needed for larger flaps including skin.
The donor site can be closed primarily if planned appropriately. Skin graft may be needed for larger flaps including skin.



2 Latissimus dorsi




 Blood Supply
Blood Supply
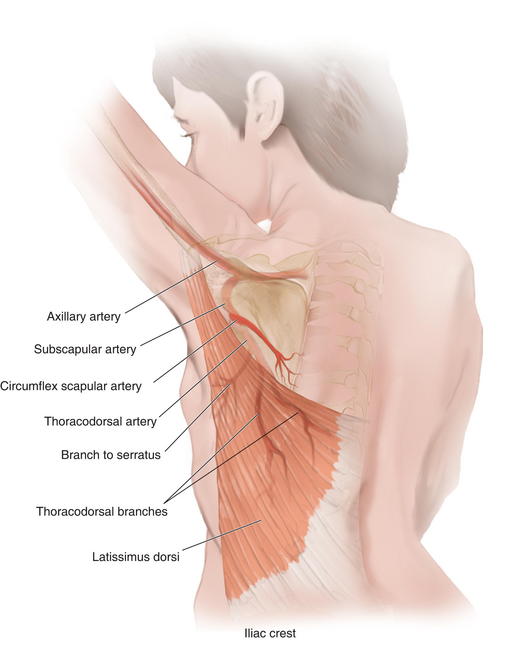
 Arterial blood is supplied through a terminal branch of the subscapular artery (2 to 5 mm diameter), a branch of the axillary artery.
Arterial blood is supplied through a terminal branch of the subscapular artery (2 to 5 mm diameter), a branch of the axillary artery. After 5 cm, the subscapular artery gives off the circumflex scapular branch posteriorly and the thoracodorsal artery (2 to 4 mm diameter) (Fig. 15-5).
After 5 cm, the subscapular artery gives off the circumflex scapular branch posteriorly and the thoracodorsal artery (2 to 4 mm diameter) (Fig. 15-5).






 Flap Design
Flap Design
 The flap design can cover ipsilateral abdominal defects. If raised as an “extended” variant, it can cross the midline by incorporating the rim of supragluteal fascia.
The flap design can cover ipsilateral abdominal defects. If raised as an “extended” variant, it can cross the midline by incorporating the rim of supragluteal fascia. If based at the muscle insertion, the pivot point is at the level of the midposterior axillary line.
If based at the muscle insertion, the pivot point is at the level of the midposterior axillary line.











