(1)
Division of Plastic-, Hand-, and Microsurgery Department of Surgery, Ludwig Maximilians University, Munich, Germany
5.1 Introductory Text
Between June 23, 1980, the first lymphatic vessel transplantation in man and January 2014 380 patients have been treated suffering from lymphedema due to a regional impairment of lymphatic flow. First results have been published in 1981 (Baumeister 1981; Baumeister et al. 1981a, b).
Most of the patients reported on previous interventions causing a local damage to the lymphatic transport system, mostly at the axilla or the groin or pelvic area.
215 patients showed a lymphedema of the upper limbs, and 155 patients suffered from lymphedema of the lower limbs. Ten patients had an edema of the penis and/or scrotum (Table 5.1).
Table 5.1
Patients treated by autogenous lymphatic vessel transplantation between June 1980 and January 2014
Autogenous lymphatic vessel transplantation | |
|---|---|
6.1980–1.2014 | |
n = 380 | |
Upper limbs | 215 |
Lower limbs | 155 |
Penis and scrotum | 10 |
5.2 Clinical Outcome in Treating Edemas of the Upper Limbs
Clinical outcome after lymphatic vessel transplantation was followed by volume measurement, lymphoscintigraphy, indirect lymphography, and quality of life assessment.
Several times, reports about actual results have been published using different evaluation methods. These are mentioned below according to the type of the follow-up method.
The actual report considers patients until January 2014.
Out of the 215 patients suffering from arm edemas, most of them, 207, were women with a history of mammary carcinoma. Only eight were man partly after mammary carcinoma too and some of them after Hodgkin treatment of Hodgkin disease. Only two patients suffered from a primary lymphedema (Table 5.2).
Table 5.2
Gender and type of patients suffering from lymphedemas of the upper limbs treated by autogenous lymphatic vessel transplantation between June 1980 and January 2014
Autogenous lymphatic vessel transplantation | |
|---|---|
6.1980–1.2014 | |
Edemas of the upper limbs | |
n = 215 | |
Female | 207 |
Male | 8 |
Primary | 2 |
Secondary | 213 |
5.3 Volume Measurements
Volume measurements were performed using the method of Kuhnke (1976). First measurements were performed prior to surgery. These measurements represented the volume achieved by the treatment with conservative means. All patients had received complete decongestive treatment (CDT) during a minimum period of 6 months. Most of the patients had undergone this kind of treatment for years. In an earlier study, the mean duration of edema prior to surgery was about 7 years.
The first publication consisted of 36 patients, all except one with postmastectomy edemas.
The mean age of the postmastectomy edema patients was 56 years, ranging from 40 to 77 years. The mean interval between mastectomy and lymphatic grafting was 10 years, ranging from 17 months to 20 years. The mean interval between the onset of edema and lymphatic grafting was 8 years, ranging from 12 months to 20 years.
The mean arm volume of 3268 cm3 preoperatively decreased to 2509 cm3 2 weeks after grafting and came down to 2436 cm3 about 2 years later. Sixteen patients with a follow-up of more than 3 years showed a mean decrease to 2195 cm3. Three years after surgery, the volumes reached an order of magnitude almost similar to those of normal arms. Over the years, the decrease in volume was not only maintained but showed further decline. The reduction reached a level of 80 % in patients with a follow-up of at least 3 years. In all groups, the stated decrease was highly significant (p < 0.001) (Baumeister and Siuda 1990).
In 2003, the results in 127 arm edemas were published. There, the mean arm volume of 3368 cm3 preoperatively decreased to 2567 cm3 around 2 weeks after grafting and was 2625 cm3 after a mean follow-up period of 2.6 years. The reduction in volume difference to the contralateral arm with a volume of 2224 cm3 was about two third (Baumeister and Frick 2003).
Through January 2014 in 214 out of the 215 patients with arm edemas, volume measurements were performed. In one patient there was no contralateral arm present.
The mean arm volume of the normal contralateral side was 2262 ± 36 cm3. The volume of the affected arm of 3288 ± 58 cm3 preoperatively decreased to 2561 ± 39 cm3 around 2 weeks after grafting and was 2634 ± 46 cm3 after a mean follow-up period of 2.5 years. Both differences are highly significant (p < 0.001) (Table 5.3, Fig. 5.1).
Table 5.3
Volume measurements in patients with arm lymphedema prior to lymphatic vessel transplantation, after hospital dismissal, and after a mean follow-up period of 2.5 years compared to the normal contralateral arm
Autogenous lymphatic vessel transplantation in edemas of the upper limbs | |||||
|---|---|---|---|---|---|
Volumes:  | |||||
n = 214 | |||||
Normal | Preop | Postop Hosp. dism. | Postop 2.5 years | p (pre/post) Hosp. dism. | p (pre/post) 2.5 years |
2262 ± 36 | 3288 ± 58 | 2561 ± 39 | 2634 ± 46 | <0.001 | <0.001 |
Fig. 5.1
Volume measurements in patients with arm lymphedema prior to lymphatic vessel transplantation, after hospital dismissal, and after a mean follow-up period of 2.5 years compared to the normal contralateral arm
Of specific interest are the changes in volume in relation to the original volume difference between the normal and the affected arm.
Regarding the 214 patients, presenting two arms, reduction in the volume difference was seen in 204 patients after a mean follow-up period of 2.5 years after lymphatic vessel transplantation. Five percent showed a minimal reduction of up to 25 %. Forty-four patients showed a reduction between 25 and 50 %. A reduction of more than 50 % was seen in 149 patients, representing more than two third of the patients. Sixty-eight out of them had a reduction between 50 and 75 %, and more than 75 % reduction was seen in 81 patients (Tables 5.3 and 5.4; Fig. 5.2).
Table 5.4
Changes in volume differences in arm lymphedema compared to the contralateral arm after lymphatic vessel transplantation
Changes in volume differences in edematous upper limbs after lymphatic vessel transplantation | ||
|---|---|---|
Difference: affected versus healthy extremity | ||
n = 214 | ||
Mean follow-up period: 2.5 years | ||
n | Percentage | |
Increase | 10 | 5 |
Reduction | ||
<25 % | 11 | 5 |
25–50 % | 44 | 20 |
50–75 % | 68 | 32 |
>75 % | 81 | 38 |
Fig. 5.2
Changes in volume differences in arm lymphedema compared to the contralateral arm after lymphatic vessel transplantation
Long-term effect of treatment is the most important factor for the patient. We grouped the patients according to minimal follow-up periods. It was shown that the effect of diminishing the volume is constant over the years with a tendency to further improvement (Table 5.5, Fig. 5.3).
Table 5.5
Long-term follow-up after lymphatic vessel transplantation in arm edemas
Autogenous lymphatic vessel transplantation in edemas of the upper limbs | |||||||
|---|---|---|---|---|---|---|---|
Volumes:  | |||||||
Minimal follow-up periods | |||||||
n | Normal | Preop | Postop | Preop | p pre/post | p pre/post | |
Hosp. dism. | Last meas. | Hosp. dism. | Last meas. | ||||
>1 year | 118 | 2190 ± 46 | 3230 ± 76 | 2531 ± 51 | 2638 ± 64 | <0.001 | <0.001 |
>3 years | 55 | 2035 ± 72 | 3044 ± 104 | 2399 ± 73 | 2461 ± 193 | <0.001 | <0.001 |
>6 years | 23 | 2000 ± 78 | 3116 ± 165 | 2405 ± 117 | 2344 ± 130 | <0.001 | <0.001 |
>8 years | 17 | 1899 ± 79 | 2855 ± 126 | 2273 ± 122 | 2220 ± 125 | <0.001 | <0.001 |
Fig. 5.3
Long-term follow-up after lymphatic vessel transplantation in arm edemas
5.4 Nuclear Medical Investigations
All patients underwent lymphoscintigraphies prior to surgery. The examination included the leg provided for harvesting and the edematous extremity. If the patient agrees, we also check the postoperative status.
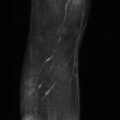
Figure 5.4 shows the follow-up of lymphoscintigraphies in a 55-year-old patient suffering from a secondary lymphedema of the left arm after mammary carcinoma before and 2, 4, and 6 years after lymphatic vessel transplantation. Prior to surgery, no activity is seen in the axilla and only a diffuse dispersion at the upper arm. After reconstruction, activity is seen corresponding to the course of the lymphatic grafts (see insert), demonstrating the transport of lymph within the grafts. The lymphatic transport index is diminished after the reconstruction, indicating the improvement in lymphatic transport.
Fig. 5.4
Example of improvement of lymphatic transport, demonstrated by lymphoscintigraphy and calculated by lymphatic transport index in a 55-year-old patient suffering from a secondary lymphedema of the left arm with a follow-up of 6 years
At different time points, the transport of lymph was followed by investigators of the Department of Nuclear Medicine at the Ludwig Maximilians University Munich.
The first investigation dated from 1985. The survey included the upper and lower extremities as well.
In 23 patients with lymphatic vessel grafts, the first medical control was undertaken at the end of hospitalization, i.e., 7–14 days after transplantation at that time. The average decrease of TI was 5.9 points. It was reduced from 31.1 points before to 25.2 points after transplantation. The corresponding volumes decreased from 3435 to 2547 ml. The changes in TI and volume were significant (p < 0.05). By comparison, the mean volume in the healthy contralateral side was 1854 ml (Kleinhans et al. 1985).
A series of patients with edemas of the upper and lower extremities and patients with primary and secondary lymphedemas was investigated in a study consisting of 20 patients (17 females and 3 males). A preoperative baseline study was compared to postoperative follow-up investigations for a period of 7 years. The reason for microsurgical lymphatic vessel transplantation was in four patients a primary and in 16 patients a secondary lymphedema. In 12 cases, the transplantation side was at the upper extremity and in eight cases at the lower limb.
In 17 out of 20 patients, the lymphatic function improved after autologous lymphatic vessel transplantation compared to preoperative findings, as verified by visual improvement of lymph drainage and decrease of numeric transport index. In five cases the vessel graft could be directly visualized. In these patients with scintigraphic visualization of the vessel grafts, the transport index decreased to a significantly greater extent compared to the preoperative baseline study. Only three patients did not benefit from microsurgical treatment (Weiss et al. 1996).
Specifically patients with arm edemas were investigated in a study with a long-term follow-up of 8 years. Twelve patients were included (age range, 32–73 years; mean age, 56 years) with secondary lymphedema of an upper extremity. All of them underwent a scintigraphic baseline study and follow-up study for a period of 8 years after microsurgical treatment.
In 11 of 12 patients, lymphatic function improved after autologous lymphatic vessel transplantation compared with preoperative findings. This could be verified by a statistically significant decrease of the transport index (p < 0.01), clear demonstration of lymph nodes, and less diffuse distribution pattern of the Tc-99 m-labeled nanocolloids. In three patients, the vessel grafts could be detected by scintigraphy (Weiss et al. 2002).
The most recent study about patients suffering from arm lymphedema consisted of 177 patients (172 females, five males; median age, 56 years, range 12–84 years) after lymphatic vessel transplantation in the upper extremity. For correlation of scintigraphic data versus reduction of volume (RV) surplus, measurements at four different time points were performed as follows: preoperatively (T0), within 2 weeks after Tx (T1), 6–12 months after Tx (T2), and 32–38 months after Tx (T3). An additional long-term follow-up after at least 8 years was available in some cases.
The maximum individual postoperative observation period was 19 years. In 169 of 177 cases, lymphedema had been caused by treatment of breast cancer (mastectomy, n = 103/169; breast preserving, n = 66/169; and/or radiation therapy, n = 130/177), but two patients presented with primary lymphedema. The remaining six cases of lymphatic disorders were caused by treatment of malignant melanoma, Hodgkin lymphoma, axillary Ewing sarcoma, non-Hodgkin lymphoma, hemangioma, or abscess removal.
At T1, the mean RV of the affected limb was 73 %, and the mean improvement of transport index (TI) was 28 %. At T2, the RV was 64 % and the TI was 23 %. And at T3, the RV was 63 % and the TI was 25 %.
Long-term follow-up after at least 8 years (T4, range, 9–19.2; mean, 14.1 years) was available in 19 of 177 patients in whom persistent improvement in the scintigraphic data (25 % decrease in TL) was confirmed by a mean clinical RV of 68 %. The mean overall correlation was by a factor of 2.64 (Weiss et al. 2015) (Fig. 5.5).
 Reconstructive Lymph Vascular Surgery and Other Lymphedema Treatment Modalities
Reconstructive Lymph Vascular Surgery and Other Lymphedema Treatment Modalities
 Pathophysiology of Lymphedemas with Respect to Surgery
Pathophysiology of Lymphedemas with Respect to Surgery
 Methods for Objectification of the Results
Methods for Objectification of the Results
 Experimental Basis of Reconstructive Lymph Vascular Surgery
Experimental Basis of Reconstructive Lymph Vascular Surgery
 Indication and Technique of Reconstructive Lymph Vascular Surgery
Indication and Technique of Reconstructive Lymph Vascular Surgery
 Venoactive Drugs
Venoactive Drugs




Related posts:
Reconstructive Lymph Vascular Surgery and Other Lymphedema Treatment Modalities
Pathophysiology of Lymphedemas with Respect to Surgery
Methods for Objectification of the Results
Experimental Basis of Reconstructive Lymph Vascular Surgery
Indication and Technique of Reconstructive Lymph Vascular Surgery
Venoactive Drugs
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
