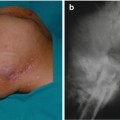
Fig. 8.1
Chronic ischial ulcer, stage IV
In an acute ulcer that develops in a short period of time, necrotic tissue is seen clinically or is covered with dry, necrotic skin (Fig. 8.2).

Fig. 8.2
Acutely developed ischial ulcer, stage IV, necrotic skin and deep tissue
The ulcer base can represent the necrotic periosteum of the ischial bone. The ulcer can extend under the gluteus maximus muscle and the hip joint, and infection can descend into the posterior thigh compartment to form a necrotizing fasciitis. Ischial ulcer can extend superiorly into the coccygeal area or inferiorly in the perineal area to involve the urethra in male patients.
8.3 Indications for Bowel Diversion (Diverting Colostomy)
There are some circumstances when bowel diversion, performed by a colostomy, is indicated before flap surgery, such as when there are multiple ulcers within the vicinity of the anus, including bilateral ischial ulcer, coccygeal ulcer, or perineal ulcer. In the author’s experience, the minimal clear distance between the flap edge and the anal verge should be at least 6 cm or more, taking into consideration the excision of the unhealthy ulcer margin during surgery. Any distance smaller than that may lead to certain morbidities in flap healing. A possible consequence of close proximity of the flap wound to the anal verge is contamination of the clean flap wound with frequent stool and the risk of bacterial colonization [1] of the wound, especially in the early stage of wound sealing. Another important consideration is mechanical interference with wound healing resulting from frequent cleaning of the anal area by nurses after a bowel program or movement that causes breaking in the wound sealing and wound sutures, which eventually causes dehesion and separation of the flap wound. The diverting colostomy became part of our preoperative requirement for these reasons. The diverting colostomy procedure can be temporary or permanent, according to the patient’s wishes. A temporary colostomy can be reversed within 6 months after flap surgery to demonstrate complete healing and no breakdown in the new flap, which indicates patient compliance to prevent flap breakdown. A double-loop type colostomy is indicated when the patient is at an end stage for flap surgery and the anus is to be closed permanently during the procedure of disarticulation and total thigh flap.
8.4 Surgery for Single Ischial Ulcer Stage IV
The following options for flap procedures can be used:
Inferiorly based gluteus maximus musculocutaneous flap (in a rotation or island sliding flap)
Hamstring muscles advancement musculocutaneous flap in V-Y closure
Gracilis muscle transfer and posterior thigh fasciocutaneous advancement flap
Gracilis muscle musculocutaneous rotation flap
Gracilis muscle transfer and medial thigh fasciocutaneous rotation flap
Gracilis muscle transfer and posterior thigh fasciocutaneous rotation flap
Gracilis muscle transfer and direct closure
Advancement of gluteus maximus flap as an island flap
A nonhealing stage III ulcer can be closed by skin graft or local fasciocutaneous flap
The choice of these options depends on many factors, including whether the ulcer is primary or recurrent, the size of ulcer, and whether the patient is ambulatory or sensory.
8.5 Gluteus Maximus Inferiorly Based Musculocutaneous Rotation Flap
8.5.1 Topographical Landmark
It is important to locate the vascular supply of the muscle on the skin surface that covers the muscle. The bony landmark is palpated and marked on the skin by a marking pen. The iliac crest, which represents attachment of the gluteal fascia or lumbar fascia where the gluteus maximus originates, and the prominent superior posterior iliac spine (PSIS), which is easy to feel in thin patients, are marked. It is sometimes not possible to feel the bone if the bone has been used previously as a bone graft in spine surgery; a scar in that area will be an indication. After location of the PSIS, a line is drawn laterally about 6 cm in length with a 45° angle from the PSIS. The end of the line represents the location of the superior gluteal artery [2]. The inferior gluteal artery and nerve are located by placing a width of about four fingers below the marked location of the superior gluteal artery in a lateral direction (Figs. 8.3 and 8.4a, b). The location of the sciatic nerve is lateral to the inferior gluteal artery and nerve.
Fig. 8.3
Topographical marking for the gluteal blood vessel, the arrow indicates the location of the superior gluteal artery
Fig. 8.4
(a) Marking the location of the inferior gluteal artery. Arrow indicates the location of the inferior gluteal artery. (b) Marking of the superior gluteal artery and inferior gluteal artery lateral view
8.5.2 Surgical Anatomy
The gluteus maximus muscle originates from many bony landmarks superiorly from the lumbar fascia, which is called the gluteal fascia below the iliac crest. The muscle originates from the sacrum at the level of the posterior superior iliac spine and the lateral edge of the lower part of the sacrum and from the coccygeal segment. The gluteus maximus muscle is inserted into a wide area, the greater trochanter, which extends into the iliotibial tract and lateral intramuscular septum (Fig. 8.5a, b). The muscle acts as an external rotator and extensor of the hip joint. It is in relationship to other muscles as its superior part covers the gluteus medius and below it covers the piriformis muscle, obturator, and quadratus femoris muscle.
Fig. 8.5
(a) Origin of the gluteus maximus muscle, sciatic nerve is lateral to the inferior gluteal artery, see arrow. (b) Origin of the gluteus maximus muscle lateral view
The sciatic nerve passes beneath the piriformis muscle and over the obturator internus muscle and obturator externus muscle. The inferior gluteal nerve originates from the sciatic nerve (L5, S1, S2), which is the motor nerve to the muscle and passes to the inferior portion of the muscle. The superior gluteal nerve supplies the gluteus medius and gluteus minimus muscle.
There are two ways to identify the plane between the gluteus maximus muscle and the gluteus medius muscle. The first approach is at the superior posterior iliac spine by detaching the muscle from that bone and passing a finger in the inferolateral direction to separate the plane between the two muscles. The confirmation that the finger is in the anatomical plane is observing the superior gluteal artery passing under the inner gluteal muscle surface. A complete detachment from the gluteal fascia superiorly and laterally from the tendinous part will then open the plane and release the muscle for medial rotation. The other is the lateral approach to the muscle by making a perpendicular incision in the skin and subcutaneous tissue and into gluteal fascia and then using electrocautery into muscle fibers until approaching the plane between the gluteus maximus and medius. The loose areolar tissue can be separated with a finger to complete the plane separation between the two muscles.
8.5.3 Vascular Pattern of the Gluteus Maximus Muscle
The gluteus maximus muscle is a dual blood supply type III muscle. The superior gluteal artery originates from the internal iliac artery. The inferior gluteal artery is located medial to the sciatic nerve. The lower portion of the gluteus maximus muscle receives additional vascular supply from the medial circumflex artery and perforator vessels from the lateral intermuscular septum of the lateral thigh compartment (Fig. 8.6).
Fig. 8.6
Vascular supply of the gluteus maximus muscle
8.5.4 Gluteus Maximus Rotation Musculocutaneous Flap
The skin territory covering the muscle has an excellent vascular supply from the muscle underneath it. It is a durable flap and is the orthodox flap for closing a single ischial ulcer in a patient without sensation or motor (i.e., nonambulatory). This flap is based on the inferior portion of the gluteus maximus muscle [3] and can be used alone or with another muscle such as the gracilis muscle. The choice of the other muscle depends on the size and depth of the ulcer and whether the ulcer is a first-time or recurrent ulcer. Some authors believe that the gluteus maximus flap should not be used for closure of ischial ulcer and should be reserved for closure of sacrococcygeal ulcers. The author’s experience is that using the inferior portion of the gluteus maximus muscle does not interfere when using the upper portion of the muscle for repair of the sacral area, whether at a later stage or simultaneously when the patient has sacral and ischial ulcer. The author has used the entire muscle simultaneously without major difficulty. The inferiorly based gluteus maximus flap can be revised and re-advanced later in case of recurrent ulceration. Lax, soft skin and subcutaneous tissue will make this revision and re-advancement easier; in a tight and scared area, it is more difficult to accomplish.
8.5.5 Flap Design
The ulcer site is marked in a triangular shape, with the apex superiorly located. A semicircular line (French curve) is drawn, extending from the lateral angle of the ulcer triangle, passing through the gluteal crease, and curving laterally over the greater trochanter. The curve extends laterally up to the level below the iliac crest and, if needed, a back cut can be made to facilitate the rotation of the flap medially to cover the defect without tension (Fig. 8.7a, b).
Fig. 8.7
(a) Flap design for inferiorly based gluteus maximus flap, patient in prone position. (b) Flap design for inferiorly based gluteus maximus flap, lateral view of the flap design
8.5.6 Operative Techniques
Excision of the ulcer and shaving of the bone are as described in Chap. 7. The skin is incised along the marked line with a scalpel, then, using an electrocautery, the subcutaneous layer and the gluteal fascia are incised, exposing the muscle fibers. The muscle fibers are incised with an electrocautery, preferably about 2–3 cm below the level of the skin incision to allow the muscle fibers, when the flap is rotated, to cover the ulcer defect. The next stage is finding the plane between the gluteus maximus and the hamstring muscle. In chronic ulceration, there is usually scarring and adhesions over the medial border of the gluteal muscle secondary to reaction from the ulcer. This scarring can be dissected down by blunt dissection to visualize the normal plane. When it is found, a finger is passed in the plane and, with the electrocautery, the transection of the muscle is completed. When approaching laterally, the plane becomes tight because of the tendinous fibers of the gluteal muscle. When the muscle approach its insertion, this needs to be incised, exposing the greater trochanter with the trochanteric bursa. The gluteus maximus fibers are then incised laterally until approaching the level below the iliac crest. The plane can be seen at this stage between the gluteus maximus and gluteus medius muscle. The flap can be lifted upward and the attached loose areolar tissue is then divided. Care should be taken to avoid injury to the hip capsule. If there are still adhesions medially near the ulcer defect, they should be divided to allow mobility of the flap. At this stage, the inferior gluteal artery should be identified passing on the posterior surface of the muscle and the sciatic nerve running laterally at the lateral border of the biceps femoris. This area is vascular and vascular injury and bleeding can occur during dissection; therefore, care should be taken to avoid this injury. The flap is rotated to cover the defect, and a check should be made to determine whether there are any tension areas. If there is a tension area medially, a back cut should be made to free the flap. Hemostasis and irrigation should be performed on the flap wound. The type of irrigation the author uses is warm normal saline mixed with an antibiotic solution such as bacitracin. If there is bleeding from the shaved ischial bone, biological collagen (Avitene®) is used to cover the bone. A good drainage system should be used to drain the area over the bone and under the flap. The exits of the drains should be away from the ulcer defect, in this case at the lateral gluteal area below the iliac crest area. The author uses closed system drains attached to a disposable electric pump (Fig. 8.8).
Fig. 8.8
Disposable electric pump drainage system (sump pump)
The closure of the flap should be done in three layers, the deep fascia and muscle using 0° Vicryl® suture, dermal layers using 3–0 Vicryl® suture, and skin with interrupted 0° polypropylene sutures. The wound is dressed with bacitracin ointment and covered with Xeroform® gauze, dry surgical gauze, and an ABD pad. A foam abduction pillow is placed between the thighs of the patient to prevent mechanical movement during nursing care in the postoperative period (Figs. 8.9, 8.10, 8.11, 8.12, and 8.13).

Fig. 8.9
Anteroposterior x-ray of the pelvis showing air over the ischium and bony changes as indicated by the arrow secondary to the ulcer
Fig. 8.10
Ulcer excised completely
Fig. 8.11
Gluteus maximus flap fully dissected and lifted upward
Fig. 8.12
(a) Operative photograph showing complete rotation of the flap to close the ulcer defect. (b) Rotation of the flap and flap sutured in place
Fig. 8.13
(a) Flap completely healed at 6 weeks post-surgery. (b) Flap healed at 6 weeks post-surgery, lateral view
8.6 Hamstring Muscle Advancement Flap
The hamstring muscle advancement flap is a musculocutaneous flap. The skin island territory of the flap is supplied with excellent perforators from the hamstring muscles beneath the skin. The muscles are the biceps femoris, semitendinosus, and semimembranous muscles [4–7]. These muscles are supplied by five main perforators from the profunda artery. The flap can be advanced to cover the ischial defect and sometimes can be rotated medially to cover some of the perineal defect. The resulting donor site of the advanced flap can be closed in a V-Y closure.
This flap is excellent for a single ulcer defect in insensate and nonambulatory patients because, when the hamstring muscles are transected distally for flap advancement, this may cause a functional deficit in ambulatory patients, especially in flexion of the knee joint. The disadvantage of this flap if the ischial ulcer does extend superiorly in the gluteal areas in this situation, technically, it is difficult to advance the flap over longer distances. Another drawback is that the proximal part of the flap, which is a few centimeters in length, is fasciocutaneous, which is not ideal for covering a deep defect. For this reason, a layer of muscle should be used first to cover the bone and the dead space and to prevent complications of a dead space. The gracilis muscle is the ideal muscle as a first layer of repair. If the gracilis muscle is not present, for example, because it has been utilized in previous surgery, the author’s recommendation is to dissect the biceps femoris muscle from the surrounding muscles and sacrifice by transect the first perforator and advance the biceps femoris muscle to cover the ischial bone and act as a first layer of repair. If the biceps muscle cannot be advanced, deepithelialization of the proximal part of the hamstring flap can be performed to create a soft tissue filler of the defects. In some circumstances, when a longer distance of advancement is required, the donor area of the flap cannot be closed with a V-Y closure and, if the closure is under tremendous tension, necrosis of the skin may result. Therefore, a skin graft is used to close the flap defect distally. The hamstring flap has excellent vascularity, which allows the flap to be revised and advanced at least twice in recurrent ulceration.
8.6.1 Surgical Anatomy
The biceps femoris muscle is the most lateral and largest of the hamstring muscles. The biceps femoris has a long and a short head. The long head of the biceps femoris and the semitendinosus and semimembranosus muscles originate from the ischial tuberosity. In extensive ulceration, the origin of these muscles will be destroyed by the ulceration and the tendinous part of the muscles becomes part of the ulcer bed and needs to be excised during ulcer excision. The short head of the biceps femoris has a deeper origin from the linea aspera of the femur. The biceps femoris is inserted distally in the head of the fibular bone and the lateral condyle of the tibia. The biceps femoris muscle is fused medially with the semitendinosus and the semimembranosus muscle through their combined origin from the ischial tuberosity in the mid-thigh area, and the sciatic nerve separates the two groups of muscles (Fig. 8.14). When the hamstring muscles are contracted, the sciatic nerve is involved with the process and becomes tight. This condition is seen frequently in paraplegic and tetraplegic patients. Therefore, advancement of the hamstring flap cannot be accomplished without transection of the muscle and the sciatic nerve. The functional importance of the biceps femoris muscle remains unclear, but it stabilizes and tightens the flexed iliotibial tract, which is an important lateral knee stabilizer. The biceps femoris muscle is a major external rotator of the knee and knee flexor in ambulatory patients and, therefore, this type of flap should not be used in ambulatory patients to avoid functional deficit.
Fig. 8.14
The anatomical relationship of the hamstring muscles
8.6.2 Vascular Supply of the Hamstring Muscles
The biceps femoris and the other hamstring muscles are a classical example of muscles supplied by segmental vessels. These deep perforator vessels at the upper two thirds of the thigh originate from the profound femoris vessel, while in the lower third of the thigh they originate from the popliteal vessel. There are total of about five perforators. In the author’s experience, the first perforator can be transected for the purpose of advancement of the biceps femoris to fill a defect in the ischial area when the gracilis muscle is not available. The motor nerve of the entire hamstring muscle is the sciatic nerve.
8.6.3 Design of the Flap
Two semi-curved lines are drawn over the posterior thigh skin, each line from each side medially and laterally of the ulcer. The two lines extend inferiorly and meet at the lower third of the posterior thigh, like a large “V.” The lateral line should not extend over the lateral intermuscular septum and the medial line should not extend into the medial thigh compartment (Fig. 8.15).

Fig. 8.15
Design of the hamstring advancement flap
8.6.4 Surgical Technique
The patient is placed in the prone position on the operating table, with the table in the jackknife position (Fig. 7.6) to ensure that, at the end of the procedure, the flap is not closed under tension. Excision of the ulcer and bone shaving are performed as described in Chap. 7. Using a scalpel, the skin is incised on each side of the v-line. The deeper tissue is incised on each side of the v-line using an electrocautery. An assistant should retract using two skin hooks, avoiding excessive pulling on the island side to prevent separation of the skin edge from the underlying muscle. When the subcutaneous layer is incised, the deep fascia that covers the muscles is exposed. On the lateral side, when the deep fascia is incised, the muscle will be exposed with freeing of the skin island. The gluteus maximus muscle superiorly should then be incised to free the flap completely and allow advancement proximally toward the defect. Medially, the fibrofatty tissue in the perineal area should be incised to expose the proximal part of the gracilis muscle and the semimembranosus muscle. In addition, the scars at the base of the ulcer should be incised to free the flap and allow medial advancement. If the flap cannot be freed to be advanced, two maneuvers can be performed to transect the hamstring muscle distally. Care should be taken not to injure the main blood vessel at the level above the popliteal fossa. The second maneuver is to release the origin of the hamstring muscle from the ischium, which allows the hamstring flap to be advanced without tension.
The author’s recommendation, as described earlier, is to use a first layer of muscle to cover the ischium. The gracilis muscle is ideal for utilization as a muscle flap through the already existing medial incision, and the gracilis tendon is transected distally and the muscle transposed to the ischial defect. Two drains should be placed, one under the muscle and the other over the muscle and the exit of these drains are at the lower part of the thigh (Figs. 8.16, 8.17, 8.18, 8.19, 8.20, and 8.21). The wound should be closed in three layers, as described previously.



Fig. 8.16
V-Y hamstring flap designed to close ischial ulcer
Fig. 8.17
The ulcer excised completely
Fig. 8.18
Operative photograph showing the hamstring flap dissected completely, the proximal part is deepithelialized and gracilis muscle utilized (long arrow), short arrow indicates the shaved ischial bone
Fig. 8.19
Advancement of the hamstring flap
Fig. 8.20
The flap is sutured in place
Fig. 8.21
Six weeks post-surgery shows complete flap healing
8.7 Gracilis Muscle Flap
The gracilis muscle flap is an excellent reconstructive option for simple, uncomplicated pressure ulcers in ambulatory and sensory patients and as a primary surgical management alternative to utilizing the gluteus maximus muscle flap or the hamstring advancement flap, reserving these flaps for recurrent ulceration or complicated cases. In the author’s opinion, the practice of using any fasciocutaneous flap (i.e., posterior thigh fasciocutaneous flap or medial thigh fasciocutaneous flap) alone is not sufficient to fill the defect and to cover the ischial bone. Utilizing the gracilis muscle is vital for immediate healing and, in the remote period, for the bone and wound healing. The gracilis muscle can be identified in surgery and it can be determined whether it has been used previously. In some instances, it can be reused to fill a defect. The gracilis muscle donor site can be closed easily. The use of the gracilis muscle has been described in the literature in closing the ischial and perineal ulcer defect [8–11]. The author’s practice is to utilize the gracilis muscle in all ischial ulcer closures when the patient is in the prone position. The contralateral gracilis muscle can be used when the gracilis of the same ulcer side was previously utilized. The contralateral gracilis can be tunneled in the perineum of the male and even in the female perineum to cover an ischial defect as a first layer.
8.7.1 Surgical Anatomy
The gracilis muscle is located in the medial thigh compartment; it is part of the adductor compartment. It is the most superficial muscle of the group and can be palpated if the patient is lying in the supine position and the hip is abducted and the knee is flexed at the same time. It originates from the pubic tubercle and the medial segment of the inferior pubic ramus. The muscle belly is flat and ends with a round tendon that is inserted in the medial surface of the upper end of the tibial body. The muscle vascularity is classified as type II. The vascular supply is a dominated artery originating from the profunda artery system as a branch from the medial femoral circumflex artery, about 8–10 cm below the pubic tubercle. At the mid and lower third of the muscle, the muscle receives one to two vascular pedicles. These are branches of the superficial femoral artery. The motor nerve supply from the anterior branch of the obturator nerve enters the muscle near the vascular pedicle entry. There are a few anatomical points that should be considered when the patient is in the prone position. The medial incision over the thigh should not be placed too medial, otherwise the gracilis muscle will be missed and the dissection is in the adductor muscle compartment. Another anatomical landmark is the long saphenous vein, which, if it is observed in the incision, indicates that the incision is too medial over the adductor muscles. To differentiate between the gracilis muscle and the hamstring muscle, one follows the origin of the muscle to confirm the identity. In addition, the gracilis muscle is smaller in size and covered with fascia. If the patient has been paralyzed for a long period of time, the muscle appearance is small and the fibers are replaced with fatty tissue. In patients with muscular spasm, the muscle will be large in volume and have hypertrophic fibers (Fig. 8.22).
Fig. 8.22
Topographical anatomy and location of the gracilis muscle. Short arrow indicates the main pedicle of the muscle, long arrow indicates the secondary pedicle of the muscle
8.7.2 Operative Technique
The patient is placed in the prone position and the operating table is in the jackknife position. Excising the ulcer and shaving the bone are performed as described in Chap. 7




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
