CHAPTER 23 Reconstruction of Malunited Ankle Fractures
DECISION MAKING AND RECONSTRUCTION
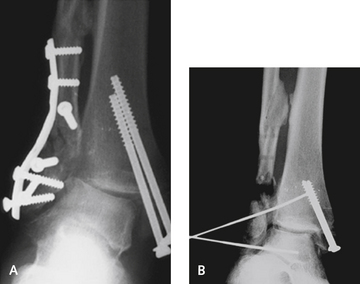
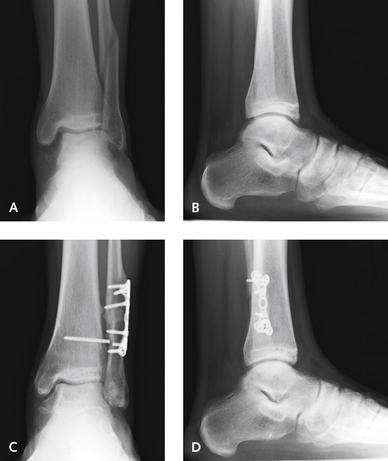
The premise for reconstruction of a malunited ankle fracture is joint preservation. Frequently, the joint may appear to be irreparable, with articular wear and erosive changes on the medial or lateral plafond. Even with these more advanced changes, however, restoring the alignment of the ankle is worthwhile. Most of these cases involve a malunion or a nonunion, or both, of the fibula. Occasionally, the medial malleolus or the posterior tibia also is involved in this malunited fracture, necessitating simultaneous correction. Lateral weight-bearing radiographs and a computed tomography (CT) scan of the ankle are helpful to plan the reconstruction. The CT scan is not necessary but does aid in determining the required degree of rotation of the fibula. It is always worth the effort to attempt a reconstruction of the malunited ankle fracture. If this fails, an arthrodesis and joint replacement are still options. The results with osteotomy of the fibula or the tibia, or both, are excellent even in ankles with considerable deformity and arthritis (Figures 23-1 and 23-2). In some situations, a reconstruction simply cannot be performed for technical reasons, and an arthrodesis is the best alternative. An important point in this context, however, is that an arthrodesis is not the only treatment option after severe trauma (Figure 23-3).


Débridement: Arthroscopy or Arthrotomy?
A decision needs to be made whether arthroscopic debridement of the joint is to be performed simultaneously. Arthroscopic evaluation of the joint is very helpful in these cases to document and stage the extent of ankle arthritis. In particular, arthroscopy is indicated for evaluation of a suspected posterior and inaccessible chondral defect that would not be visible with anterolateral arthrotomy. The hypertrophic tissue between the medial malleolus and the talus must be excised from the medial gutter for the reposition of the talus. Surprisingly small amounts of tissue in the medial gutter can actually block the correct medial shift of the talus back into the mortise (Figure 23-4). Fibular malunion generally is associated with a lateral translational deformity of the talus with an increase in the medial clear space, and the medial joint recess must be debrided, under visualization afforded by either arthrotomy or arthroscopy.
Fibular and Medial Malleolus Deformity and Osteotomy
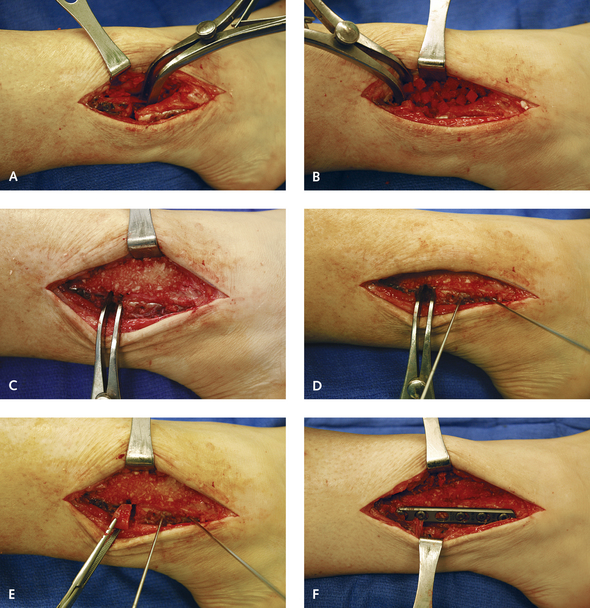
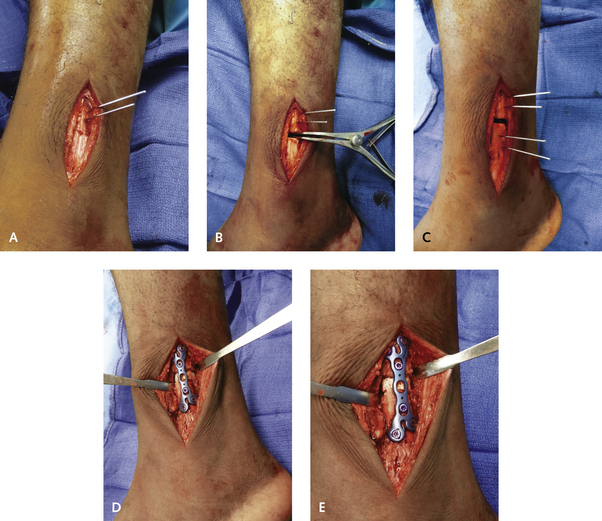
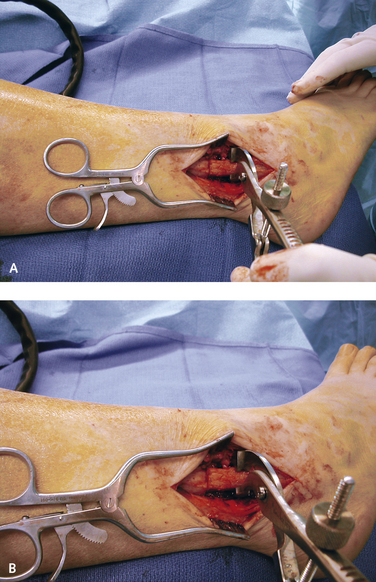
The fibula is commonly shortened and externally rotated in a malunion, although only one of these may be present, determining the type of osteotomy and bone graft. Ideally, it should not be necessary to strip the entire syndesmosis in order to lengthen the fibula. In cases in which the syndesmosis must be included in the procedure, such as arthrodesis requiring creation of a tibia pro fibula, then the syndesmosis should be taken down completely (Figures 23-5 and 23-6). If the fibula is externally rotated and not shortened, then a derotational osteotomy can be performed without lengthening, thereby preserving the syndesmosis (Figure 23-7).