(1)
Yotsuya Medical Cube, Chiyoda-ku, Tokyo, Japan
Basic Principles
The first choice procedure for reconstructing the thumb tip is a palmar advancement flap, and by expanding the flap as far as the thenar, it is possible to cover an even larger skin defect.
For finger tip defects other than the thumb,
For transverse amputation, an oblique triangular flap or palmar flap advancement are indicated.
For oblique amputations on the palmar side, as long as the skin defect area doesn’t exceed the DIP joint, a reverse flow digital arterial flap is indicated. For a large defect that exceeds the distal phalanx area, either a hemi pulp transfer or reverse flow digital arterial cross finger flap is indicated.
All palmar advancement flaps include the nerves in the flap. For reverse vascular pedicle digital island flap, thenar flap or hetero digital island arterial flap, because similar tissue is used, it is not essential to include sensory function. The cross finger flap from the dorsum of the finger replaces tissue with tissue of a different quality, so this cannot be a first option. However, when skin of a different quality must be used for the reconstruction of a fingertip, sensory function should be reconstructed at the same time (in the case of a cross finger flap, the dorsal branch of the digital nerve in the flap is sutured to the digital nerve in the recipient site).
Selectable Flaps and Surgical Procedures
Palmar advancement flap of thumbHemi pulp transferHetero digital arterial flap from ring fingerOblique triangular flapReverse flow digital arterial flapThenar flapHemi pulp transferReverse flow digital artery cross finger flapHeuston’s flap modificationUlnar parametacarpal flapGraft-on flap methodNail bed graft from great toe on flapTissue banking using insertion in subcutaneous pocketThe difficulty level of each surgical procedure is shown subsequent to the procedure title (e.g., Level of Difficulty: 2). The levels range from 1 to 5, with level 1 indicating a preliminary level and level 5 indicating a very advanced level.

8.1 Oblique Triangular Flap Modification (Level of Difficulty: 3)
Information
Vascular pedicle Digital arterial neuro pedicle
Size The distal skin flap is the same width as the longitudinal axis (short pedicle) of the finger amputation stump, and length extends to the PIP joint.
Indication The flap transfer distance is 10–15 mm
Caution In the conventional design, the width of the flap was made the same as the transverse diameter of the amputation stump, and the flap was simply advanced distally. Using this method, the nerve end was located at the distal end of the finger, and patients complained of stump pain post operation. In this modification, the width of the flap is the longitudinal diameter of the finger amputation stump, and a long narrow flap is used to cover the finger amputation stump while being rotated (rotate advancement).
Also, regardless of the size of the area to be covered, by dissecting a long neurovascular pedicle for the flap down to the base of the finger, it is possible to remove tension and reduce numbness and pain of the finger tip following surgery.
Because the path of the arterial neuro pedicle of the finger is moved forward following transfer of the flap, it is necessary to dissect a sufficient amount of the subcutaneous tissue in the volar center of the finger so that the neurovascular pedicle can be transferred to the volar center without being pulled tight.
8.1.1 Operation Procedures

Fig. 8.1
Procedure 1: A transverse amputation of the nail bed area of the left index finger
Note
In order to includSe a nerve in the skin flap, elevation of a skin flap from the radial side of the index finger, the radial side of the middle finger, or the ulnar side of the little finger, should be avoided.


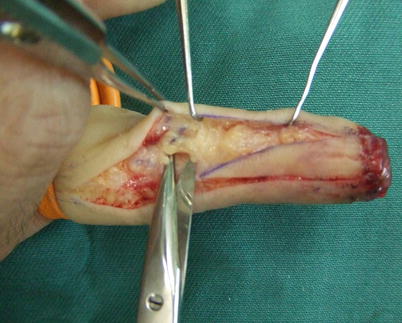
Fig. 8.2
Procedure 2: First, a line is drawn along the full length of the mid-lateral line of the finger, and the width of the distal end of the flap is decided by the longitudinal diameter of the finger amputation stump. From that point a line is drawn diagonally to the PIP joint, and a long narrow flap is designed
Fig. 8.3
Procedure 3: An incision is made in the margin of the flap. A deep incision is made in the line along the mid-lateral line of the finger down to the periosteum, and a shallow incision is made subcutaneously along the diagonal line
Fig. 8.4
Procedure 4: The digital neurovascular pedicle is identified in the distal area of the flap and broadly dissected, with the surrounding fat included. Also, the flap is broadly dissected subcutaneously moving from the flap margin to the center of the finger
Note
Because the path of the neurovascular pedicle of the finger is moved forward following transfer of the flap, it is necessary to dissect a sufficient amount of the subcutaneous tissue in the center of the finger so that the neurovascular pedicle can be transferred without being pulled tight.
(Part of photos reproduced from Hirase, Y. Secrets to successful graft on flap: plastic surgery – Knacks and pitfalls of hand surgery. pp 282–284, Bunkodo, 2007)
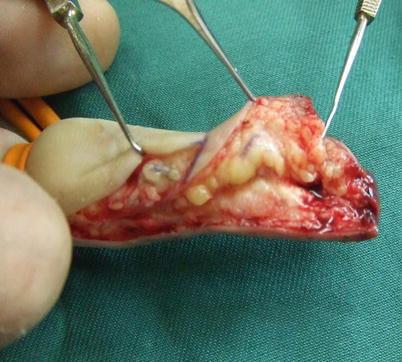
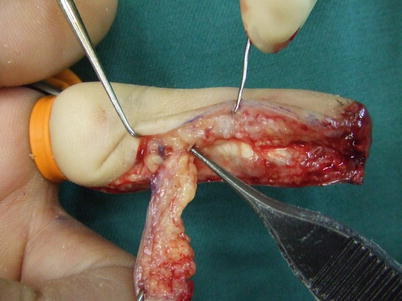
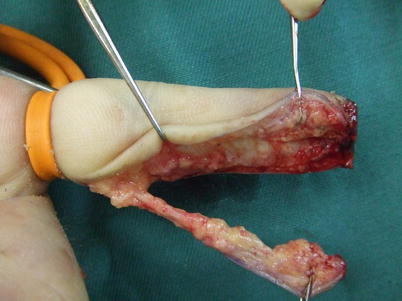
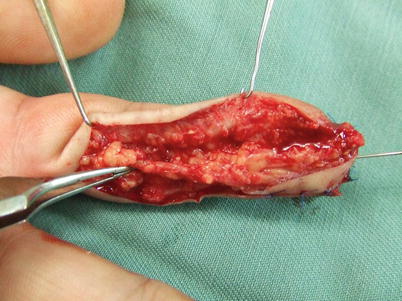


Fig. 8.5
Procedure 5: The flap is dissected from the layer above the tendon sheath. When the flap is turned over it is possible to identify the vascular pedicle on the reverse side, and dissection is continued using that as a guide
Fig. 8.6
Procedure 6: A large amount of peripheral fat is attached to the vascular pedicle of the flap, which is elevated as a thick pedicle
Fig. 8.7
Procedure 7: A long length of vascular pedicle is detached down to the base of the finger
Fig. 8.8
Procedure 8: The tourniquet is released and the circulation of the blood flow is confirmed. The skin flap is rotated and advanced to distal to cover the finger tip. The skin flap is fixed in place using a Kirschner wire inserted into the fingertip. From this procedure, the neurovascular pedicle has been transferred from its original path to the volar center
Fig. 8.9
Procedure 9: The skin flap is sutured to the surrounding area
Fig. 8.10
Procedure 10: By rotating and transferring the flap, it is possible to form sufficient bulge in the volar fingertip. The incision line does not cross the DIP or PIP crease so there is no new scar contracture. (Part of photos reproduced from Hirase, Y.: Treatment of nail and fingertip injuries (6) using free flaps. MB Orthop 20:81–87, 2007)
Tips
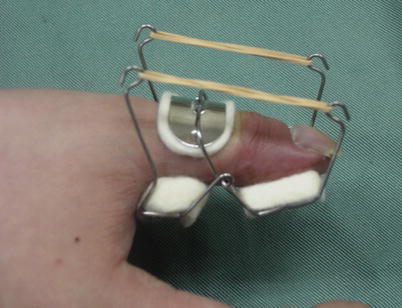
Use a finger extensor device at 2 weeks following surgery to prevent flexion contracture
In order to prevent flexion contracture of the IP or PIP joint following flap surgery, a finger extensor device should be fitted at 2 weeks following surgery
8.2 Graft-on Flap Method by Oblique Triangular Flap (Level of Difficulty: 3)
Information
Indication Cases involving finger amputation at the nail bed level where re-attachment is considered difficult
Advantage Short operating time, and surgical technique is comparatively simple.
Caution The transplant tissue mustn’t become dry. Early stage debridement is not performed.
8.2.1 Operation Procedures

Fig. 8.11
Procedure 1: Case of complete amputation of the nail area of the finger
Fig. 8.12
Procedure 2: Amputated section of finger includes part of the distal phalanx
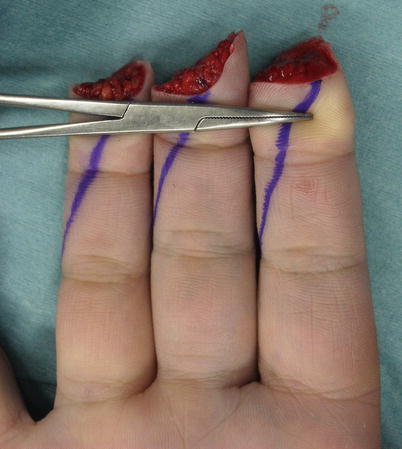
Fig. 8.13
Procedure 3: An oblique triangular flap is designed
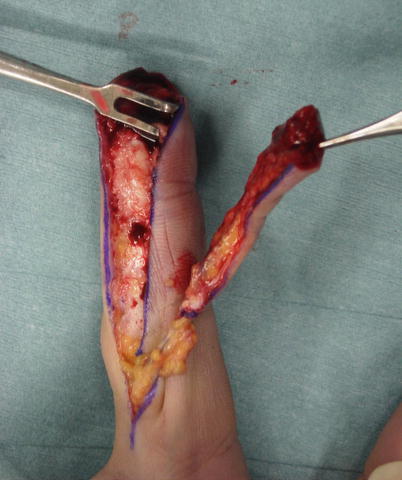
Fig. 8.14
Procedure 4: An oblique triangular flap is elevated
Refer to Section of
“Reconstruction of fingertip/Oblique triangular flap modification” in Chap. 8



Fig. 8.15
Procedure 5: Flap is used to reconstruct the palmar side of the fingertip
Fig. 8.16
Procedure 6: Appearance of the dorsal fingertip after reconstructing the fingertip using the flap
Fig. 8.17
Procedure 7: Only the bone and the nail bed are harvested as a single entity from the amputated section of the fingers
Note
If a large amount of soft tissue is included in the tissue transplanted from the amputated finger, the take ratio is decreased. It is important that when conducting a transplant like a skin graft that the tissue is as thin as possible, and that soft tissue other than the nail bed is decreased as much as possible. For that reason, it is necessary to create a graft with sufficient size on the palmar side for conducting the reconstruction.

Fig. 8.18
Procedure 8: The bone is fixed in place with a thin wire (0.7 mm), and the nail bed is sewn in place with careful alignment using an absorbable suture. The surrounding skin is also sutured
Fig. 8.19
(a, b) Procedure 9: Appearance immediately after surgery
Note
It took 92 min to reattach the three fingers.
Liberal amounts of ointment are continually applied to the transplanted nail bed to prevent it from drying out, and the scab is not removed for 2 weeks.

Fig. 8.20
(a, b) Procedure 10: Appearance of nails 1 year later. Healthy nail growth can be seen. The bulge on the palmar side of the fingertip has been accurately recreated. Return of sensory function is also recognized
Fig. 8.21
Procedure 11: X-ray image 1 year after surgery. No bone absorption in the finger tip. (Some photos reproduced from Hirase, Y., et al.: A new reattachment procedure for fingers amputated at the nail bed level. Journal of Japanese Society for Surgery of the Hand 20:501–504, 2003)
Tips
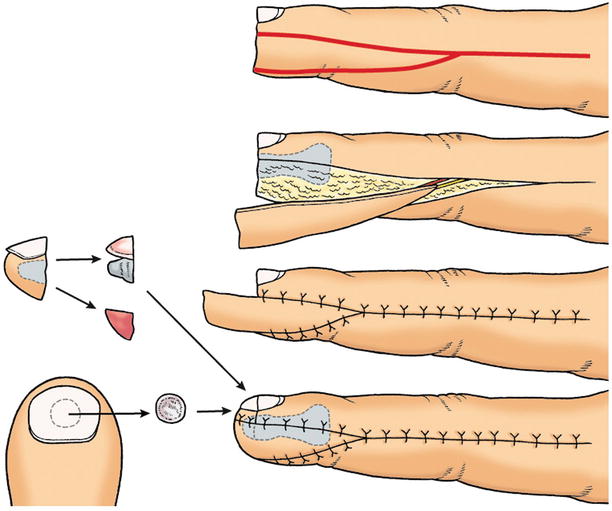
Concept of graft-on flap method
The basic concept of the graft-on flap method is reconstructing the palmar side of the finger using a flap, and transplanting the nail bed onto that. Therefore, the requirement is that even though the nail bed is lost, the nail matrix still remains. In emergency amputation cases, the nail bed is harvested from the amputated fingers, but for mature amputation cases or fingertip deformation cases the nail bed is harvested from the nail bed of the great toe.
8.3 Extended Palmar Flap Advancement with V-Y and Z Plasty (Level of Difficulty: 2)
Information
Vascular pedicle Digital artery
Size The flap is designed from the palmar side of the thumb to the thenar.
In order to obtain a greater transfer distance, the design of the flap is extended to the proximal thenar. V-Y plasty is conducted in the proximal area of the flap.
Indication Digital arteries to the thumb is inserting from the ulnar side at the mid- point of the ulnar side of thenar region. Therefore, if the flap is designed extending to the thenar region over the insertion of digital arteries, the digital arteries are not pulled by moving the flap, but the flap is rotated without tension of digital arteries as the pivot point. It is possible to create a complete island flap by dissecting the flap from the tendon sheath, the flap can be moved more than 2 cm
Caution When creating an advanced thenar flap, several Z plasties should be conducted to prevent a new contracture from occurring on the margins of the flap.
8.3.1 Operation Procedures

Fig. 8.22
Procedure 1: Case of skin defect on palmar thumb tip. A thumb palmar advancement flap that extends to the proximal thenar is designed, and a Z plasty is planned for the margin in line with the finger crease, following movement of the flap. The entire proximal area of the flap is to be closed using a V-Y plasty, and a Z plasty is added to the tip
Note
The solid line in the flap shown in the photo is to be moved to the dotted line following movement of the flap, and a Z plasty is conducted here (solid line outside the flap).

Fig. 8.23
Procedure 2: An incision is made in the flap margin, and the flap is detached above the tendon sheath, however as far as possible, the dorsal branch from the digital artery is retained
Note
For the thumb, even if all of the dorsal branch of the digital artery is severed, necrosis of the skin on the dorsum of the finger does not occur. But for other than the thumb, if the entire dorsal branch is severed, then this can cause skin necrosis on the dorsal side of the distal phalanx.


Fig. 8.24
Procedure 3: The flap is completely detached from above the tendon sheath, creating a complete island flap elevated with only the digital nerve and vascular pedicle
Fig. 8.25




Procedure 4: After the skin flap is moved distally, V-Y plasty is conducted to the proximal end and Z plasty conducted to the margins to close the wound
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
