(1)
Yotsuya Medical Cube, Chiyoda-ku, Tokyo, Japan
Basic Principles
The distal 1/3 of the lower leg has a tendency for an open fracture or osteomyelitis to occur, and it can be difficult to obtain skin/muscle flap with vascular pedicle from the affected limb due to a lack of blood vessel length. Therefore, this is an area with good indication for use of free muscle and musculocutaneous flaps, but there is a higher possibility of thrombus occurring compared to the upper limb. To address this issue, anastomosis is conducted for the posterior tibial arterial system using end-to-side anastomosis as the method.
End-to-side anastomosis is also useful for retaining blood flow in the affected limb.
When performing free tissue transplant, posterior tibial artery end-to-side (side-to-side) anastomosis is the main method of anastomosis, and is conducted in the popliteal region or medial malleolus region.
Selectable Flaps and Surgical Procedures
Free latissimus dorsi musculocutaneous flap/serratus anterior muscle flapFree gastrocnemius muscle flapReverse flow sural artery skin flapBi-pedicle skin flapReverse turn-over fascial flapExtensor digitorum brevis muscle flapCross leg flap methodPeroneal artery flapFree scapular/parascapular flapThe difficulty level of each surgical procedure is shown subsequent to the procedure title (e.g., Level of Difficulty: 2). The levels range from 1 to 5, with level 1 indicating a preliminary level and level 5 indicating a very advanced level.

16.1 Reverse Turn-Over Fascial Flap (Level of Difficulty: 2)
Information
Vascular pedicle Mainly superficial sural artery, peroneal artery and partial use of branch from posterior tibial artery
Size Superior margin 3–5 cm distal from popliteal crease; inferior margin 6–8 cm proximal from medial and lateral malleolus. Fascial flap made to size required to fit 10–15 cm width for this area. An overlap margin of 5 cm from the wound is secured.
Advantage Fascia is thin, flexible and strong. Can perform surgery in same operating area. Surgery is extremely easy. No complex techniques are required
Disadvantage A skin graft is required
16.1.1 Operation Procedures

Fig. 16.1
Procedure 1: Based on size of skin defect area, design consisted of leaving at least 5 cm of lower calf fascia without detaching, securing an overlap of the same length, and enabling removal of fascia the size of the skin defect area from the proximal end
Refer to Section of
“Reconstruction of Achilles tendon area/Reverse turn-over fascial flap” in Chap. 17


Fig. 16.2
Procedure 2: An incision is made into the skin on the posterior lower leg, and the fascia exposed
Fig. 16.3
Procedure 3: The fascia, based on the design and including the overlap, is detached and elevated from the posterior lower leg. If the sural nerve cannot be retained, then it is severed and included in the fascial flap
Fig. 16.4
Procedure 4: The fascia flap is turned over from the posterior lower leg toward the distal anterior lower leg
Note
Make sure not to detach areas that need to be retained.


Fig. 16.5
Procedure 5: The exposed bone area is covered using the fascia flap, and a bolster suture conducted to pull the muscle flap into the subcutaneous layer
Fig. 16.6
Procedure 6: A split-thickness skin graft is conducted over the fascia, and a tie-over bolster dressing is applied. Fixed using a plaster splint
Tips
If negative pressure wound therapy is performed instead of a tie-over bolster dressing, then a splint is not required.

16.2 Reverse Flow Sural Artery Skin Flap (Level of Difficulty: 2)
Information
Vascular pedicle Superficial sural artery accompanying the sural nerve that runs along center of posterior lower leg. When creating a reverse skin flap, the sural nerve and small saphenous vein are included.
Size Width about 5 cm; length is length of sural nerve without restriction
Advantage Technique is simple and surgery time is short
Disadvantage Due to bending of broad skin flap and pedicle, there is tendency for vascular insufficiency to occur. The skin flap can also become thick depending on transfer direction.
Caution Obtain blood vessels from a wide area, not only for the skin flap pedicle

16.2.1 Operation Procedures

Fig. 16.7
Procedure 1: The osteomyelitis region of the distal area of right medial lower leg is debrided, and sustained release antibiotic hydroxyapatite (Boneceram-P ®) inserted

Fig. 16.8
Procedure 2: In prone position, the skin flap axis is established in the center of the posterior lower leg. The flap pivot point is set at 5 cm proximal from the lateral malleolus, and the skin flap is designed above the sural nerve and small saphenous vein (center of posterior lower leg) using the same distance as the distance from this point to the skin defect area

Fig. 16.9
Procedure 3: The subcutaneous tissue is gradually exposed while making sure that the skin flap is comprised of the superficial sural artery accompanying the sural nerve, and is above the small saphenous vein. The fascia pedicle of the skin flap is created with 3 cm width
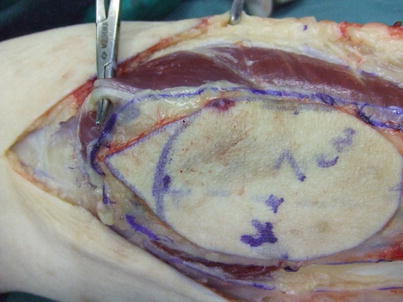
Fig. 16.10
Procedure 4: The small saphenous vein is ligated at the proximal end, and the artery accompanying the sural nerve severed

Fig. 16.11
Procedure 5: The flap pedicle is detached in the distal direction beneath the fascia and the skin flap elevated. The tourniquet is released and reverse blood flow to the skin flap confirmed

Fig. 16.12
Procedure 6: The skin flap is transferred to the skin defect area through the subcutaneous tunnel, and a bolster suture conducted to pull the muscle flap into the subcutaneous layer
Note
If the subcutaneous tunnel is not created large enough it will apply pressure to the vascular pedicle of the skin flap.

Fig. 16.13
Procedure 7: A split-thickness skin graft is conducted on the donor area
Tips
Flap congestion improves after a few days, however edema persists for several weeks
Mild congestion and edema tends to occur in the skin flap for several days following surgery.