(1)
Yotsuya Medical Cube, Chiyoda-ku, Tokyo, Japan
Basic Principles
Materials for reconstructing skin defects in the Achilles tendon area need to form thin and strong skin flaps. There is no need for sensory function.
The first consideration is reconstruction with a local flap using skin from the area surrounding the defect, but in many cases this is difficult because of crushing injury to the surrounding tissue.
As an arterial island flap, medial pedis flap, a reverse peroneal flap and a lateral calcaneal flap using a V-Y shape are the most practical. This can mean that the operating area becomes much larger, but combining the lower calf fascia as a turn-over fascial flap and a skin graft is a simple and stable procedure. As the free tissue transfer, either of a temporal fascia flap or a combination of a muscle flap and a skin graft, that decreases in by atrophy, is an excellent choice. A free musculocutaneous flap is too thick and not suitable. If a free skin flap is chosen, a flap should be selected where thinning is possible.
In the case of transplanting free tissue, end-to-side anastomosis is performed to the posterior tibial blood vessels in the medial malleolus region.
Selectable Flaps and Surgical Procedures
Medial pedis flapLateral calcaneal flap (conventional method)Lateral calcaneal sliding flapReverse flow peroneal flapReverse turn-over fascial flapReverse flow sural arteryskin flapSupra malleolar flapFree temporal fascia flapFree abdominal perforator flapFree latissimus dorsi musculocutaneous flap (serratus anterior muscle flap) transferThe difficulty level of each surgical procedure is shown subsequent to the procedure title (e.g., Level of Difficulty: 2). The levels range from 1 to 5, with level 1 indicating a preliminary level and level 5 indicating a very advanced level.

17.1 Lateral Calcaneal Flap (Conventional Method) (Level of Difficulty: 2)
Information
Vascular pedicle Lateral calcaneal artery (Mostly distal end of peroneal artery. At times the distal end of the posterior tibial artery is used, but it is always available)
Size width 4–5 cm, length 8–15 cm
Advantage Similar texture, has sensory function
Disadvantage Skin graft is required for donor site closure but it is difficult to take.
Donor site scar is obvious
(Reproduced from Yuichi Hirase, et al.: Long-term follow-up of a patient with lateral calcaneal flaps for bilateral posterior heel necrosis. Ann Plast Surg 26: 474–478, 1991)

17.1.1 Operation Procedures

Fig. 17.1
Procedure 1: The position of the lateral calcaneal artery is confirmed prior to surgery using the Doppler blood flow measurement, and the skin flap is designed slightly longer than the necrotic area between the lateral malleolus of the fibula and the Achilles tendon
Note
When the reconstruction area for the Achilles tendon extends to the heel, a longer skin flap that curves slightly forward is designed. The patient is often in the equinus position when the design is being conducted, so a ruptured suture can easily occur at the flap edge following surgery. Therefore it is essential to create a longer skin flap in consideration of correction of the position of the feet.

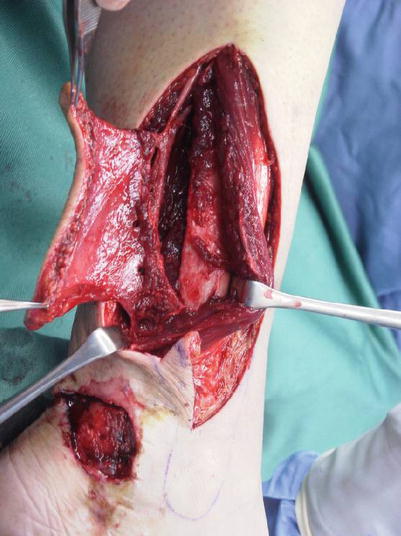
Fig. 17.2
Procedure 2: Patient is placed in the lateral recumbent position or abdominal position. Incision is made from the distal end of the flap, and the flap dissected from above the periosteum. The skin flap is elevated towards the proximal end while confirming the blood vessels and nerves on the reverse side of the flap
Note
The lateral calcaneal artery runs above the periosteum. Because it runs along the thick part of the tissue and not directly underneath the skin flap, it gives an impression that the distal part of the flap is comparatively thick, but if the artery is not fully included then an arterial flap cannot be created.


Fig. 17.3
Procedure 3: The skin flap is transferred above the necrotic area and sewn in place. Care is taken to make sure the ankle joint is not in the equinus position
Fig. 17.4
Procedure 4: A split-thickness skin graft is conducted on the donor site, and a tie-over bolster dressing applied. A cast is applied to the lower leg
Note
Although there are few problems with the flap itself following surgery, with regard to the skin graft to the donor site, because the graft is conducted directly onto the periosteum, hematoma tends to occur beneath the skin graft, and occasionally it is difficult to take. It is preferable to leave the cast on for 2–3 weeks following surgery. In the case that it doesn’t take, multiple skin grafts can at times be required.
Tips
The disadvantage of the lateral calcaneal flap is the donor site
Grafting is conducted directly above the periosteum, and if there is incomplete pressure, a hematoma can tend to occur.
A small hole is opened in the skin graft so that hematomas can be discharged, pressure applied and plaster left on for longer than usual.
Although the depression that forms at the donor site improves over the longterm, a comparatively obvious scar remains. For small skin defects of the Achilles area, a lateral calcaneal sliding flap using a V-Y form is preferred.
17.2 Lateral Calcaneal Sliding Flap (Level of Difficulty: 3)
Information
Vascular pedicle Lateral calcaneal artery
(Mostly distal end of peroneal artery. At times the distal end of the posterior tibial artery is used, but it is always available)
Size Width 3–5 cm, length 5–8 cm
Advantage Similar texture, has sensory function. Skin graft is not required.
Disadvantage The transfer distance for the flap is short, and is not suitable for covering large areas.

17.2.1 Operation Procedures

Fig. 17.5
Procedure 1: A triangular flap is designed adjacent to the skin defect area on the Achilles tendon
Note
This is to be kept in mind when deciding the width of the flap for enabling the nutrient vessel to run between the Achilles tendon and the lateral malleolus of the fibula. It is possible to determine for certain if confirmed using a Doppler blood flow measurement.

Fig. 17.6
Procedure 2: An incision is made surrounding the flap, and the lateral calcaneal artery & vein running above the periosteum confirmed. The proximal and distal sections of the vascular pedicle of the skin flap are confirmed and retained and the skin flap completely dissected from the surrounding area
Note
In many cases the sural nerve also runs alongside. The vascular pedicle is deep and runs above the periosteum.

Fig. 17.7
Procedure 3: The skin flap is transferred laterally in accordance with the V-Y plasty technique, and sutured to the surrounding area
Tips
The first choice skin flap when reconstruction areas are not too large
In this case the skin texture with the surrounding skin is extremely good, and the inconspicuousness of the scar tissue after reconstruction is striking. The area of surgery is small, and the volume of blood loss is also minor. However the vascular pedicle is at a deep layer above the periosteum, so it is necessary to elevate a thick skin flap. Do not dissect the thinner layer.

17.3 Reverse Peroneal Flap (Level of Difficulty: 4)
Information
Vascular pedicle Peroneal artery and its skin perforator
Pivot joint Difficult to increase to a more distal position than 5–6 cm proximal of the lateral malleolus of the fibula
Size width 10 cm; length 20 cm
Advantage Skin texture is similar. Can perform surgery in same operating area.
Disadvantage If skin flap is large, skin graft becomes necessary and is obvious.
17.3.1 Operation Procedures
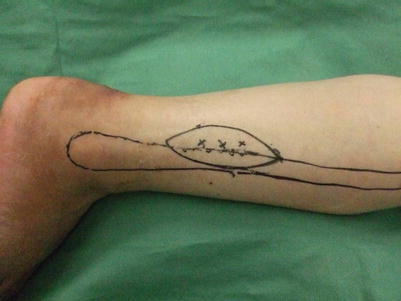
Fig. 17.8
Procedure 1: In prone position, prior to surgery, Doppler measurement is conducted of the perforators of the peroneal artery positioned at the rear margin of the fibula, distal of the middle of the lower leg, and the peroneal flap is designed with that cutaneous branch included. Surgery is performed under a tourniquet
Note
Ordinarily 3–4 perforators to be included in the skin flap, are located at intervals of 2–3 cm from the middle of the fibula. Perforators proximal from the middle of the fibula are perforators for the muscle and not for the skin, so even if they are picked up by Doppler measurement, they cannot be used for a vascular pedicle for the skin flap.

Fig. 17.9
Procedure 2: An incision/detachment is made to the anterior margin of the skin flap (front of fibula) including the deep fascia and the front section of the skin flap elevated. It is then possible to confirm the perforators heading toward the skin through the thin fascia at the rear margin of the fibula
Note
The skin perforators rise up from behind the skin, so it is possible to confirm the perforators when starting to elevate the front margin of the flap.
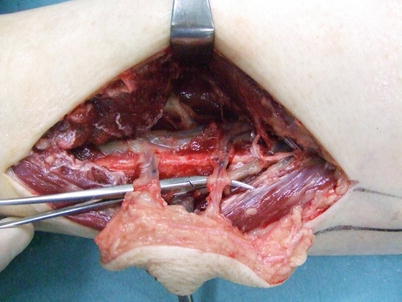
Fig. 17.10




Procedure 3: An incision is made in the posterior margin of the flap, and the flap dissected from the soleus muscle with the soleus fascia attached on the flap side. When the soleus muscle is moved aside the flexor hallucis longus muscle can be seen. The fibula blood vessels that become the vascular pedicle for the skin flap, are located in this flexor hallucis longus muscle, so with care, the vascular pedicle on the posterior side of the fibula are detached
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
