, Paul N. Chugay1 and Melvin A. Shiffman2
(1)
Long Beach, CA, USA
(2)
Tustin, CA, USA
Abstract
The authors focus on the treatment of volume deficiency of the anterior thigh, particularly that associated with HIV and HAART regimens. There is a discussion of the basic anatomy of the region, the preoperative marking of the patient, and the operative procedure. Postoperative care is described as well as potential postoperative complications with a discussion of observed complications and the management of those complications. There is a brief discussion of highly active antiretroviral therapy (HAART) associated and HIV muscle wasting syndrome.
Introduction
Solid silicone prostheses have been used in multiple areas of the body to give volume to an area that is devoid of substance either due to trauma or post-oncologic procedures and in those who suffer from hypoplasia of a given muscle group due to congenital myodystrophies. In the past decade, it has been the experience in the author’s practice that patients are seeking for ways to bulk up further in muscle regions that may be unresponsive to conventional exercise routines. Recently, patients with HIV or on highly active antiretroviral therapy (HAART) have presented to the author’s practice seeking bulk in areas that have been ravaged by muscle wasting. It was to that end that a custom silicone implant was devised for a patient to treat muscle wasting in the anterior thigh, which he found particularly vexing.
To further expand the use of a quadriceps implant, one may consider its use in patients that are fit but wish to further enhance the volume in the anterior compartment of the thigh. The quadriceps muscles make up the majority of the volume in the anterior thigh. A person that wishes to increase volume in the anterior thigh has to do more than just cardiovascular work but has to take time and focus in on building up the quadriceps muscles [1]. Many trainers and bodybuilding authors agree that an intensive bodybuilding routine is required to build muscle in the anterior thigh; for some, the intensity of this routine may be prohibitive in getting a “bulked up” quadriceps region.
Indications
Quadriceps augmentation surgery is indicated in patients that have a defect in the anterior thigh region after trauma or post-oncologic procedures. It is also indicated for augmentation of the anterior thigh due to muscle wasting. Finally, there may be a role for quadriceps augmentation in patients who persistently have hypoplasia of the anterior thigh and wish to have an enlarged thigh volume for cosmetic reasons.
Contraindications
Patients with HIV or on immunosuppression therapy are at increased risk of infections. This must be considered in counseling patients for surgery involving muscle implants. Furthermore, an HIV patient with a high viral load is likely not a good candidate as their systemic illness is not well controlled and may put them at risk for increased complications post-op.
Limitations
The current quadriceps implant does not alter the appearance of the vastus lateralis or medialis as it has not been developed to be that large in size and its augmentation scope is limited to the area immediately above the rectus femoris and vastus intermedius.
Relevant Anatomy
The quadriceps femoris (Latin for “four-headed muscle of the femur”) is a large muscle group that includes the four prevailing muscles on the front of the thigh: rectus femoris, vastus lateralis, vastus intermedius, and vastus medialis (Fig. 10.1). These muscles act as the primary extensor muscles of the knee and form the volume of the anterior thigh region, overlying the femur. The quadriceps femoris is located in the anterior compartment of the thigh which is bounded by the inguinal ligament superiorly, the capsule of the knee inferiorly, the iliotibial tract laterally, and the femoral neurovascular bundle medially. The fascia overlying the muscles of the anterior compartment is divided into superficial and deep layers. The superficial fascia forms a continuous layer over the whole of the thigh. It consists of loose areolar tissue which is intermingled with fat. Deep to this is the deep investing fascia of the thigh. The deep fascia of the thigh is commonly referred to as the fascia lata. Just like the superficial fascia, it varies in thickness in different parts. It is thicker in the upper and lateral part of the thigh, where it receives a fibrous expansion from the gluteus maximus and where the tensor fasciae latae is inserted between its layers. It is very thin behind and at the upper and medial part of the thigh, where it covers the adductor muscles, and again becomes stronger around the knee. The anterior thigh is relatively free of neurovascular structures, with the majority of structures being deep to the femur or localized to the upper medial thigh (Fig. 10.2). The greater saphenous vein is transmitted through the superficial and deep layers of fascia at the fossa ovalis, located in the upper medial thigh. It is below the deep layer of fascia that the saphenous vein joins the femoral vessels and saphenous nerve (Fig. 10.3) [2]. With the proposed dissection for the anterior quadriceps augmentation, these structures are free from the risk of injury.
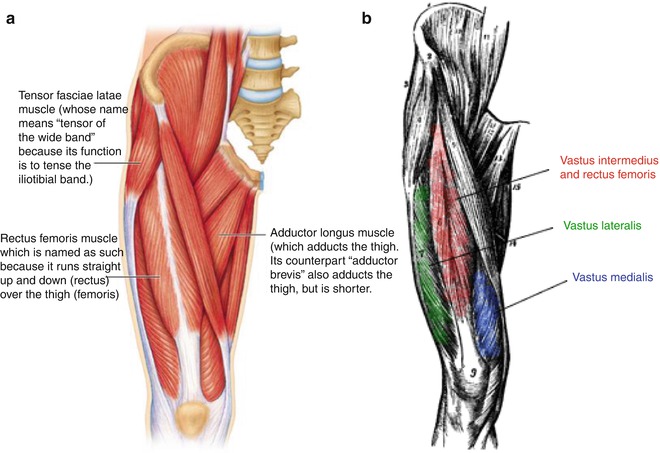
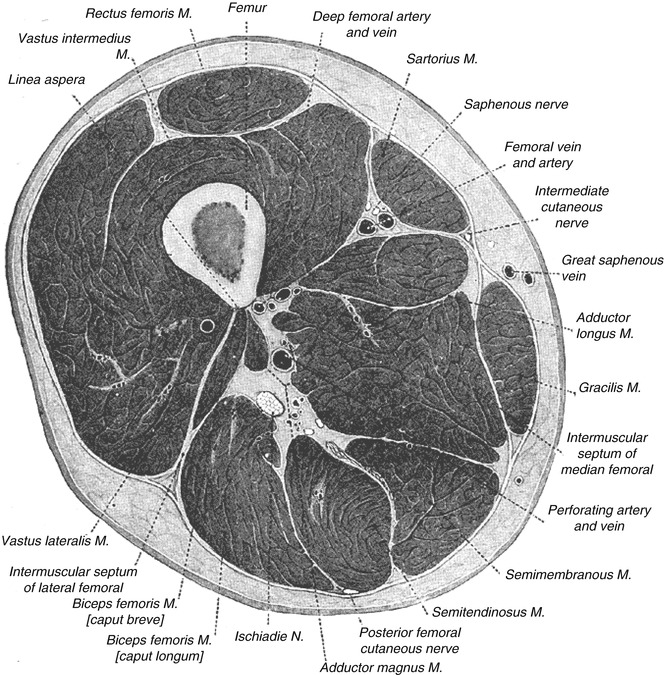

Fig. 10.1
Muscles of the anterior thigh
Fig. 10.2
Cross section through mid-thigh. Note the absence of major neurovascular structures in the area of the anterior thigh
Fig. 10.3
Greater saphenous vein emptying into the femoral vein at the fossa ovalis in the medial thigh
Consultation/Implant Selection
A thorough history and physical are paramount to preventing complications at the time of quadriceps augmentation. For patients that do present with HIV or on HAART, further investigation regarding the state of their immunodeficiency should be made. If available, the patient’s CD4 count should be requested. An inquiry into any remote or recent infections is made. Questions are posed regarding the patient’s reasonable attempts to build the muscle with conventional means. If the patient is suffering from muscle wasting, then there should be an assessment of the reason for the wasting (e.g., muscular dystrophy, muscle wasting of HIV/HAART, inactivity, etc.). During the consultation, patient’s expectations are managed and assessment of the patient’s mental state is undertaken. It is made clear to the patient the expected augmentation that can be seen with augmentation and limitations of the procedure are also explained.
After completion of the history portion of the consultation, an evaluation of the patient’s thigh is made. Any asymmetries or defects are pointed out to the patient. The patient’s muscles are then evaluated. The skin and fat content are similarly assessed at this time as a patient with minimal adipose and thin skin is more at risk for implant palpability. Measurements of the patient’s thighs are then taken: (1) circumference of the thigh at its midpoint and (2) length from the inguinal crease to the patella to ascertain the maximal size of the implant.
Available Implants: Custom-Made for Implantation by Dr. Chugay
The dimensions of the implant used for augmentation are as follows: 10.4 × 15 × 2.5 cm (Fig. 10.4).

Fig. 10.4
Preoperative marking with location of incision and proposed site of implant
Preoperative Planning and Marking
On the day of the surgery, the patient is met in the preoperative holding area. It is here that the patient’s consent is verified and again risks, benefits, and alternatives are reviewed with the patient. With the patient in the erect position, the proposed site of incision is marked, measuring approximately 5–7 cm. The site of incision should be in the upper thigh, approximately 8–10 cm below the inguinal crease (Fig. 10.5). Once the site of the incision is marked, the site of the proposed implant is marked taking into account the patient’s anatomy and existing deficit along with the desires of the patient.
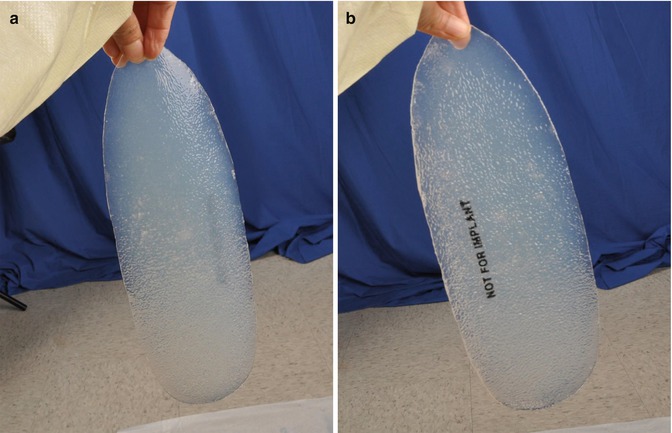
Fig. 10.5
(a, b) Second generation quadriceps implant for implantation custom-made for Chugay cosmetic. The tapered end (being held) would be placed caudally and the wider portion of the implant cranially, conforming to the normal anatomy of the leg. This implant has not yet been placed but has been created to fill out a larger area of the anterior thigh
Operative Technique
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


