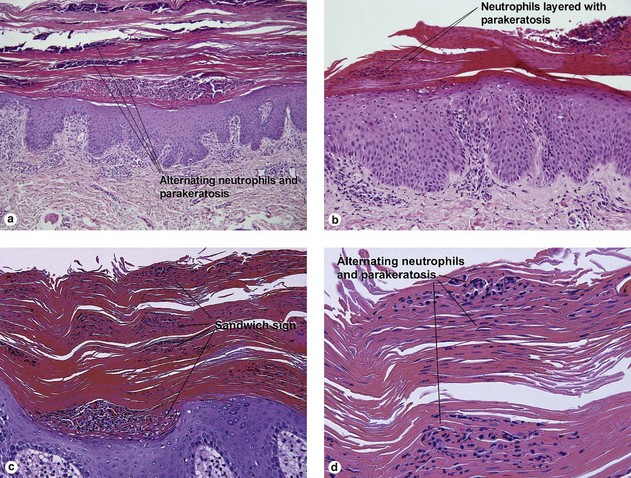
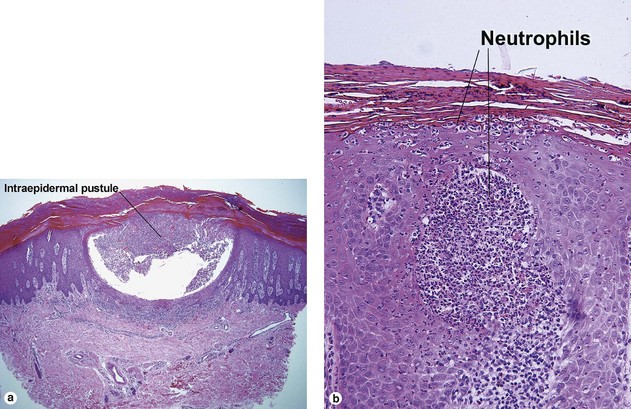
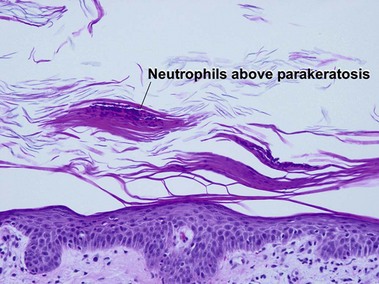
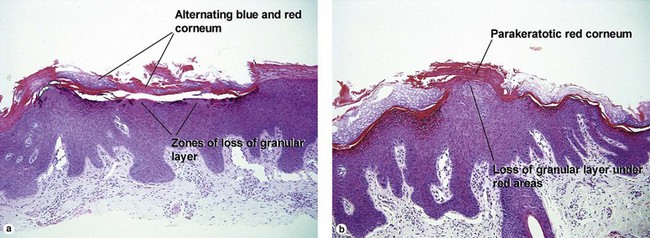
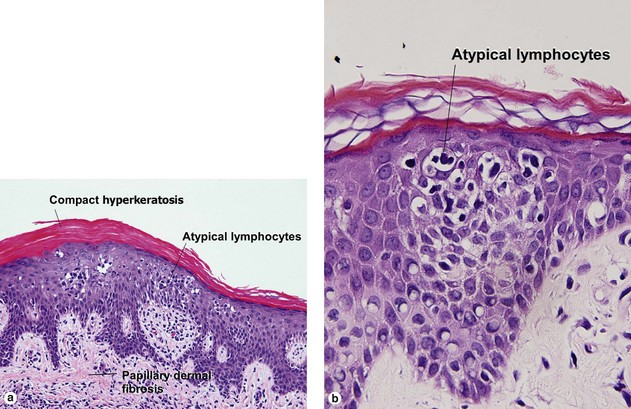
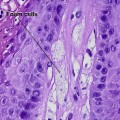
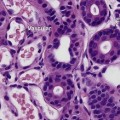
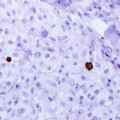
Chapter 8 Psoriasiform and spongiotic dermatitis Dirk M. Elston Psoriasis Key features • Neutrophils above parakeratosis in stratum corneum • Little to no serum in stratum corneum • Alternating neutrophils and parakeratosis in the stratum corneum (sandwich sign) • Neutrophilic spongiform pustules • Little spongiosis in adjacent epidermis • Tortuous blood vessels in dermal papillae The appearance of psoriasis depends on the stage of the lesion and type of lesion. Early guttate lesions demonstrate no acanthosis. Established plaques demonstrate a characteristic pattern of regular acanthosis. Pustular psoriasis may never demonstrate acanthosis. Acral and intertriginous lesions of psoriasis commonly demonstrate a background of spongiosis, but spongiosis is distinctly absent from the surrounding epidermis in most other locations. Reiter’s disease and geographic tongue histologically look like psoriasis. Pearl Collections of neutrophils within the stratum corneum: • Psoriasis, tinea, impetigo, Candida, seborrheic dermatitis, syphilis (PTICSS) Plaque psoriasis Key features • Regular bulbous club-shaped acanthosis • Thin superpapillary plates • Alternating neutrophils and parakeratosis in the stratum corneum (sandwich sign) • Little to no serum in stratum corneum • Neutrophilic spongiform pustules • Little spongiosis in adjacent epidermis Fig 8-1 Plaque psoriasis Pustular psoriasis Key features • Collections of neutrophils within stratum corneum • Subcorneal pustules • Spongiform pustules Fig 8-2 Pustular psoriasis Pearl Subcorneal pustules: Candida, acropustulosis of infancy, transient neonatal pustular melanosis, Sneddon–Wilkinson (and IgA pemphigus), impetigo, pustular psoriasis, Staphylococcus scalded-skin syndrome (CAT SIPS, or an anagram of SIPS) Guttate psoriasis Key features • Neutrophils above parakeratosis The key histologic feature of guttate psoriasis is a focus of neutrophils on top of parakeratosis (half of the sandwich sign, jelly up). The neutrophilic focus may be small and only visible in step sections. The focus often has a hump-like configuration or resembles a child’s drawing of a seagull. Fig 8-3 Guttate psoriasis Inflammatory linear verrucous epidermal nevus (ILVEN) Key features • Alternating ortho- and parakeratosis from left to right • Areas of orthokeratosis have a prominent granular layer • Areas of parakeratosis lack an underlying granular layer (see Chapter 2) Fig 8-4 Inflammatory linear verrucous epidermal nevus (ILVEN) Mycosis fungoides Key features • Epidermal collections of lymphocytes • Lymphocytes hyperchromatic and surrounded by white space (lump of coal on a pillow) • Epidermal lymphocytes larger, darker, and more angulated than lymphocytes in dermis • Little spongiosis in adjacent epidermis • Papillary dermal fibrosis • In areas, lymphocytes may also line up along the dermal epidermal junction • Bare underbelly sign (see Chapters 7 and 24) Fig 8-5 Psoriasiform mycosis fungoides Syphilis Key features • Vacuolar interface dermatitis together with elongated psoriasiform acanthosis • Vacuolar interface dermatitis together with interstitial dermal infiltrate (busy dermis) Only gold members can continue reading. Log In or Register to continue Related Related posts: Key diagnostic features of additional soft tissue neoplasms Bacterial, spirochete, and protozoan infections Alterations in collagen and elastin Granulomatous and histiocytic diseases Sweat gland neoplasms The basics: Diagnostic terms, skin anatomy, and stains Stay updated, free articles. Join our Telegram channel Join Tags: Dermatopathology Apr 26, 2016 | Posted by admin in Dermatology | Comments Off on Psoriasiform and spongiotic dermatitis Full access? Get Clinical Tree Get Clinical Tree app for offline access Get Clinical Tree app for offline access
Chapter 8 Psoriasiform and spongiotic dermatitis Dirk M. Elston Psoriasis Key features • Neutrophils above parakeratosis in stratum corneum • Little to no serum in stratum corneum • Alternating neutrophils and parakeratosis in the stratum corneum (sandwich sign) • Neutrophilic spongiform pustules • Little spongiosis in adjacent epidermis • Tortuous blood vessels in dermal papillae The appearance of psoriasis depends on the stage of the lesion and type of lesion. Early guttate lesions demonstrate no acanthosis. Established plaques demonstrate a characteristic pattern of regular acanthosis. Pustular psoriasis may never demonstrate acanthosis. Acral and intertriginous lesions of psoriasis commonly demonstrate a background of spongiosis, but spongiosis is distinctly absent from the surrounding epidermis in most other locations. Reiter’s disease and geographic tongue histologically look like psoriasis. Pearl Collections of neutrophils within the stratum corneum: • Psoriasis, tinea, impetigo, Candida, seborrheic dermatitis, syphilis (PTICSS) Plaque psoriasis Key features • Regular bulbous club-shaped acanthosis • Thin superpapillary plates • Alternating neutrophils and parakeratosis in the stratum corneum (sandwich sign) • Little to no serum in stratum corneum • Neutrophilic spongiform pustules • Little spongiosis in adjacent epidermis Fig 8-1 Plaque psoriasis Pustular psoriasis Key features • Collections of neutrophils within stratum corneum • Subcorneal pustules • Spongiform pustules Fig 8-2 Pustular psoriasis Pearl Subcorneal pustules: Candida, acropustulosis of infancy, transient neonatal pustular melanosis, Sneddon–Wilkinson (and IgA pemphigus), impetigo, pustular psoriasis, Staphylococcus scalded-skin syndrome (CAT SIPS, or an anagram of SIPS) Guttate psoriasis Key features • Neutrophils above parakeratosis The key histologic feature of guttate psoriasis is a focus of neutrophils on top of parakeratosis (half of the sandwich sign, jelly up). The neutrophilic focus may be small and only visible in step sections. The focus often has a hump-like configuration or resembles a child’s drawing of a seagull. Fig 8-3 Guttate psoriasis Inflammatory linear verrucous epidermal nevus (ILVEN) Key features • Alternating ortho- and parakeratosis from left to right • Areas of orthokeratosis have a prominent granular layer • Areas of parakeratosis lack an underlying granular layer (see Chapter 2) Fig 8-4 Inflammatory linear verrucous epidermal nevus (ILVEN) Mycosis fungoides Key features • Epidermal collections of lymphocytes • Lymphocytes hyperchromatic and surrounded by white space (lump of coal on a pillow) • Epidermal lymphocytes larger, darker, and more angulated than lymphocytes in dermis • Little spongiosis in adjacent epidermis • Papillary dermal fibrosis • In areas, lymphocytes may also line up along the dermal epidermal junction • Bare underbelly sign (see Chapters 7 and 24) Fig 8-5 Psoriasiform mycosis fungoides Syphilis Key features • Vacuolar interface dermatitis together with elongated psoriasiform acanthosis • Vacuolar interface dermatitis together with interstitial dermal infiltrate (busy dermis) Only gold members can continue reading. Log In or Register to continue Related Related posts: Key diagnostic features of additional soft tissue neoplasms Bacterial, spirochete, and protozoan infections Alterations in collagen and elastin Granulomatous and histiocytic diseases Sweat gland neoplasms The basics: Diagnostic terms, skin anatomy, and stains Stay updated, free articles. Join our Telegram channel Join Tags: Dermatopathology Apr 26, 2016 | Posted by admin in Dermatology | Comments Off on Psoriasiform and spongiotic dermatitis Full access? Get Clinical Tree