CHAPTER 4 Proximal Phalangeal Osteotomy (Akin Osteotomy)
Although used predominantly for correction of symptomatic hallux valgus, this osteotomy is useful in conjunction with correction of a crossover second toe deformity, even when the hallux valgus is asymptomatic. The second toe is difficult if not impossible to realign if the hallux is abutting it laterally, because there is no room to correct the toe deformity and reposition the toe without underriding of the toe by the hallux, leading to recurrent deformity. Correction of the mechanical axis of the hallux MP joint also is important, for example, with an abnormal distal metatarsal articular angle. Correction of the MP joint alignment abnormality with a biplanar osteotomy of the distal first metatarsal is preferable. With the addition of the phalangeal osteotomy, however, the hallux shortens slightly. As a result, tension on the extrinsic tendons decreases, and correction of the pronation is easier. Although the closing wedge phalanx osteotomy is of secondary importance, it does improve the cosmetic appearance of the toe. The phalangeal osteotomy is very useful to correct fixed pronation of the hallux. This deformity does not correct well with any osteotomy, and trying to pull the capsule using the capsulorrhaphy to correct the pronation does not work (Figure 4-1).

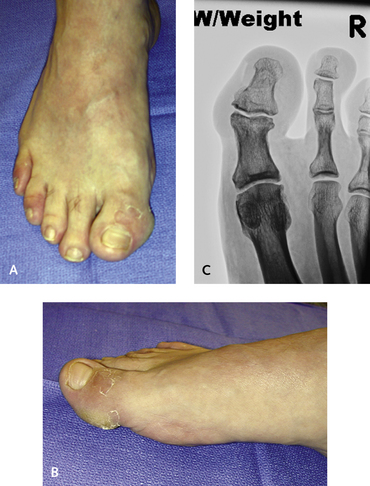
The traditional use of the phalangeal osteotomy is to function as an adjunctive procedure for the correction of hallux valgus. As discussed further on, this osteotomy is performed in the metaphysis at the base of the proximal phalanx. A far more important use of the phalangeal osteotomy, however, is the correction of hallux valgus interphalangeus (Figures 4-2 and 4-3). Other than an arthrodesis of the hallux interphalangeal (IP) joint, the only method of correction that will work is an osteotomy through the distal portion of the proximal phalanx.