Fig. 17.1
A computerized pressure mapping of an individual sitting on a Jay 2 cushion. The dark blue indicates areas of low pressure (<10 mmHg). The red indicates areas of high pressure (>100 mmHg)
Identifying potential risks already in his/her environment and then brainstorming solutions with the patient will increase his ability to identify other risks that he/she may encounter.
17.3 Special Beds and Positioning
If an individual has good skin integrity, a supportive mattress should be sufficient with proper turning for pressure relief. For those individuals who are not able to turn themselves, it is necessary to look at other alternatives. One alternative is prone positioning (Fig. 17.2).
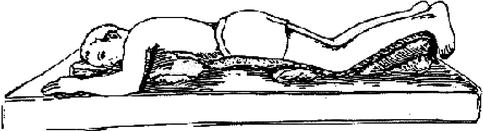
Fig. 17.2
A person in prone position, pillows placed under the chest and thighs to eliminate pressure over anterior iliac crest, the thighs and lower leg to eliminate pressure on the knees, and dorsum of the foot to eliminate pressure on toes
A patient can lay on the stomach with pillows positioned under his/her chest, hips, thighs, and anterior lower leg to bridge the hip bone, knee, and dorsum of the foot. In order to sleep this way, most individuals will need to be able to freely move his/her head so that breathing is easy. Most individuals with paraplegia or lower level tetraplegia can be in a prone position. It may be important to show the patient how to set up his/her pillows, and some patients may need to work on progressing to a full night’s sleep in this position. A higher level of tetraplegia with weakened neck muscles or individuals with fusions and limited range of motion will have difficulty in this position. For these individuals, alternative mattress options will need to be explored. Water beds that are appropriately filled can reduce peak pressure and provide good pressure distribution; it is important that the water level be appropriate as too low can lead to bottom to firm surface and too high could increase peak pressure and lead to ulcers [4]. It is also important with the water bed to assess that the individual can transfer from it without shear or trauma to the skin during transfer. Low air loss mattress will provide for good pressure distribution and may allow for longer time before the patient needs to be repositioned; however, they do not eliminate the need for turning. For the individual that cannot position in prone and does not have the ability to turn himself/herself, a turning or alternating air mattress may be a better option. The Volkner System® has been tested in our facility and has been an effective product for home use to assist our clients who need a turning mattress at home (Fig. 17.3).

Fig. 17.3
The Volkner Alpha® mattress overlay for home use. It alternates a person’s position over time to reduce prolonged pressure over bony areas
It is important for the patient to be able to try this mattress to ensure that they can sleep on it and that the mattress provides effective pressure through the night. Additionally, an individual that develops a pressure ulcer may need to use an air mattress to assist with healing if prone positioning is not an option.
As an individual is more at risk for pressure ulcers after an initial occurrence, it is important that the medical staff take the necessary steps to prevent pressure ulcers when patients are in acute care and long-term care settings. There has been an increased awareness of pressure ulcers in the acute care setting with greater emphasis on prevention in recent years. Most hospitals have guidelines in place to assess individuals at risk for pressure ulcers. Once an individual at risk has been identified, it is important that that individual be placed on a turning schedule (at least every 2 h), that he/she is not bowel or bladder incontinent, and if so, that prompt hygiene is performed to prevent skin maceration and breakdown. There are a variety of beds that can be used in this setting to assist with the prevention of pressure ulcer. The standard mattress will produce greater than 30 mmHg over the bony areas in supine, specifically the sacrum/coccygeal area, heels, and scapula. A low air loss bed will provide a reduction of pressure and improved body contact to improve pressure distribution (Fig. 17.4).

Fig. 17.4
Flexicare Eclipse® from Hill-Rom®. This is an example of low air loss mattress used at the 4 weeks post flap wound care in the pressure ulcer management unit. It reduces peak pressure allowing a patient to stay in one position longer prior to being turned. This reduction reduces risk but a patient will still need periodic turning to eliminate risk for pressure ulcer
There are several different manufacturers of low air loss beds, but essentially the bed uses air as flotation device to provide full contact throughout the body surface and reduced pressure over peak areas; the air system can also be monitored for temperature control. Ryan et al. found that the low air loss mattress greatly reduced pressure over all bony surfaces in an individual in a supine position, with the exception of the occiput. The pressure over the occiput was still much lower than the standard bed but had higher pressures than other bony surfaces [4].
The use of the turning mattress is becoming more common in hospitals and long-term care facilities. The Volkner Alpha® (Fig. 17.3) is an example of a turning mattress that can be used at home. The turning mattress will alternate pressure from one side to the other, effectively turning the individual from side to side. It is important to monitor the individual’s position to ensure that he/she is maintaining position at the center of the bed. The rotation cycle varies from different manufacturers and can be programmed in some. The turning mattress is especially important for the acute care setting where pain or severe medical complications may limit the ability to turn a patient effectively, for example, a tetraplegic patient on a mechanical ventilator. A turning mattress may also be a solution to managing a bariatric patient to reduce the risk of injury to the staff.
17.4 Sitting Pressure Management
A person that uses a wheelchair for mobility will need to have his/her seating system evaluated. The individual should be educated on the importance of each piece of equipment from the upholstery to the footrest to the cushion. He/she should be educated on the importance of sitting alignment on pressure distribution and assisted in identifying other areas that he/she may sit. Does he/she transfer to the couch for family time or to watch the game? Does the couch bottom out when he/she sits on it? Is he/she doing pressure relief when sitting? What is the frequency of his/her pressure relief? Does it change when he/she is sitting on different surfaces? In every place that he/she sits, does he/she need to do pressure relief? If the surface is harder than his/her cushion (i.e., padded toilet seat), should he/she do pressure relief more frequently? As part of our rehabilitation program, the occupational and physical therapists discuss a patient’s typical and atypical day. We go on outings and have discussions to assist the patient in identifying their own risk factors and ways to reduce them.
Pressure relief (eliminating the pressure over bony areas) is a component of pressure management that needs to be addressed routinely. It is important that the patient understands that there is always a need to do pressure relief and give several options on how to perform pressure reliefs in a variety of settings. Pressure relief in sitting needs to be done every 15–30 min [2, 4]. The recommendation from the rehabilitation team following reconstructive surgery is every 15 min when sitting in the prescribed seating system. Sitting on a surface that is not their prescribed seating system should warrant even more frequent pressure relief and should only be done when necessary and for short period of time. For example, when sitting on the toilet to complete bowel program, the toilet seat should be padded, but this will not distribute pressure as well as his/her own cushion; therefore, pressure relief should be done more frequently to prevent pressure ulcers. Whenever possible an individual should sit on his/her own cushion, for example, if he/she transfers to the couch to sit with his/her family, he/she should transfer his/her cushion to the couch and sit on it or into the car seat. Pressure relief should be done in all of these activities.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


