8 Phenol Peeling
Introduction
The distribution of peel patients used for this chapter are seen in Table 8.1. Factors affecting phenol peel depth are shown in Box 8.1. One hundred and fifty-nine full face phenol peels and nine human biopsy studies were used in this study. Results of these efforts were published in Clinics in Plastic Surgery.
Table 8.1 Distribution of peel patients in this study
| Formula | Number of patients | Age range |
|---|---|---|
| Venner-Kellson | 18 | 29–60 |
| Maschek-Truppman | 7 | 46–63 |
| Finsti | 3 | 55–65 |
| Baker-Gordon w/o croton oil | 1 | 60 |
| Gradé I | 3 | 46–49 |
| Gradé II | 4 | 40–48 |
| Gradé III | 2 | 41–64 |
| Stone II | 24 | 32–72 |
| Combined Gradé II, III | 2 | 47–49 |
| Combined Gradé I, III | 3 | 38–64 |
| Combined Gradé III, Baker-Gordon | 1 | 57 |
| Combined I, II, Baker-Gordon | 1 | 47 |
| Combined Gradé II, Stone II | 3 | 31–52 |
| Stone II-Venner-Kellson | 23 | 42–71 |
| Combined Stone II, Baker-Gordon | 2 | 38–49 |
| Combined Baker-Gordon, Venner-Kellson | 4 | 28–60 |
| Combined Baker-Gordon, Venner-Kellson, TCA | 1 | 71 |
| Combined Baker-Gordon, TCA | 2 | 56–60 |
| Combined Maschek-Truppman, Baker-Gordon | 1 | 58 |
| Combined Venner-Kellson, TCA | 6 | 28–69 |
| Baker-Gordon | 48 | 29–74 |
| Total | 159 |
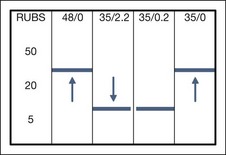
Based on these studies and two new experiments reported below, the author concluded that: (1) rubbing increased the depth of injury (agree with Hetter); (2) the thickness of papillary dermis injury, the degree of fibrosis, and the degree of inflammation were less with 5 rubs and more with 50 rubs (Fig. 8.1); (3) phenol is not all-or-none (agree with Hetter); (4) croton oil increased depth of injury (agree with Hetter); (5) there was little observable difference between 0.4% croton oil and 2.2% croton oil when application techniques were kept constant (disagree with Hetter), and (6) human experimental models have inherent variables.
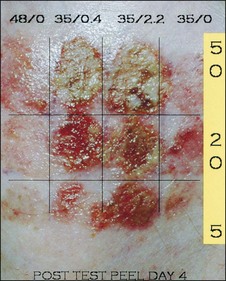
Based on quantifiably reproducible experimental test peel patch studies on the right cheek and, later, left cheek test peel patches (reported below), using 48% phenol with 0.0% croton oil, 35% phenol with 0.4% croton oil, 35% phenol with 2.2% croton oil, and 35% phenol with 0.0% croton oil (see Fig. 8.1), a lowering of the threshold affect to create injury (Fig. 8.2) to between 5 and 20 rubs can be seen when croton oil is added. This is down from the 20 to 50 rubs required when croton oil is excluded. The early appearance of coagulation is not a true indicator of depth of peel, nor is the immediate density of frost as evidenced by the reported superficial results from 88% USP Phenol which can produce an immediate, dense, white frost. The length of time a given formula is applied, the concentration of phenol and croton oil, the volume of acid, the vigor and abrasiveness of the application and predegreasing procedure, and the occlusive technique all play a vital role in the final result.
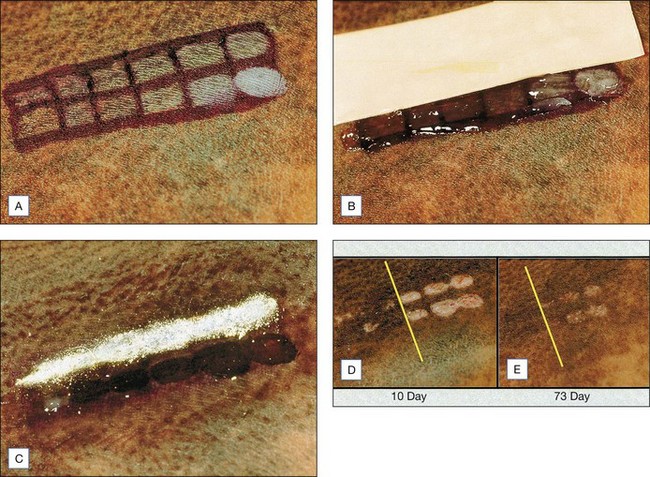
In order to further test the hypothesis that length of application or number of rubs plays a paramount role in peel result, an African-American male, age 37, with a truncal congenital nevus of Becker was tested with one formula: the Stone II (60% phenol, 0.2% croton oil) (Fig. 8.3A–E). Twelve test patches, six in each of two rows, were rubbed with 1, 5, 10, 20, 50, and 100 coats using twice-blotted, semi-dried Q-tips. The top row was covered with tape for 48 hours followed by thymol iodide powder (Delasco Laboratories, Council Bluffs, IA) for 7 days. The bottom row was covered with Aquaphor ointment until healed. A clear threshold between 10 and 20 rubs was seen by day 10 and persisted through to day 73, the last day of the study.
Based on this objective data, it is the author’s conclusion that both the Hetter and Stone techniques can produce excellent results with modified phenol. The student is left with a clear choice. Using the Hetter technique the student will employ several dilutions over multiple facial and neck zones with an ointment occlusion, or will choose one formula with a timed application and a waterproof tape/ powder occlusion. It is a bit like comparing proven facelift techniques. Not one method is good for all students or all patients. See Box 8.2 for key features.
Box 8.2
Key features
Treatment Approach
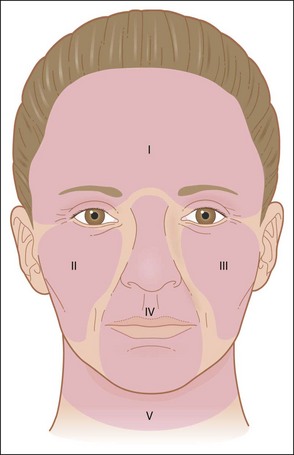
• Definition of zones
It is a well known fact that a thorough phenol peel should take a minimum of 1 hour to avoid too rapid absorption of phenol. Therefore, the face is divided into zones for the purpose of ensuring that the procedure takes a minimum of 90 minutes to complete (Fig. 8.4).