19 Perioral filling
Summary and Key Features
• The perioral region is particularly susceptible to the signs of aging
• Biodegradable fillers can improve the appearance of vertical lip rhytides, oral commissures, and the chin and jawline
• Permanent fillers should not be used in the lips
• Fillers are often combined with neuromodulation to control movement and increase longevity of the filling agent in the lower face and in the lips
• Conservative treatment with small doses is recommended
• Many complications can be avoided by careful injection techniques and suitable product selection
Anatomical considerations
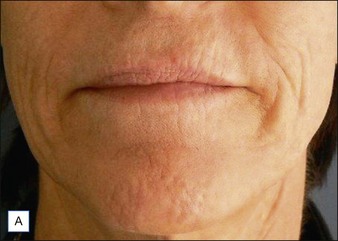
Age-related changes are a result of a combination of factors, including loss of subcutaneous volume, thinning of the dermis, changes in bony structures, skin laxity due to loss of collagen and elastin, and downward gravitational shift of the skin and underlying tissues. Over the years, the entire perioral region begins to droop. The lips may deflate and flatten, vertical rhytides appear above and below the vermilion lips, the mandible rotates (downward and backward for women; forward for men), and oral commissures turn down emphasizing the drooping mouth and prominence of the marionette lines. Soft tissue atrophy and bone reduction in the region between the chin and jowl result in a groove termed the pre-jowl sulcus. Redistribution of overlying skin and subcutaneous tissues results in the underprojection of the chin and malar eminences. Loss of definition occurs around the mandible, and the mentalis area develops a pebbled ‘peau d’orange’ appearance owing to repetitive muscular activity in conjunction with volume loss in the chin (Fig. 19.1).

Injection techniques
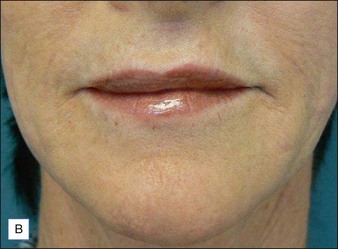
Like the choice of appropriate filling agent, injection techniques vary. Initial patient evaluation should include an overall assessment of the diffuse volume deficit, as well as the individual lines and depressions for a multifaceted treatment approach (Fig. 19.2). In some cases, rejuvenation of the lower face can be accomplished with filling agents alone using a conservative approach and follow-up visits to assess the need for additional treatment. Because of the dynamic nature of the perioral region, fillers often do not last as long as they do in less mobile locations. For this reason, restoration of volume in the lower face is often combined with movement control via botulinum toxin (BoNT). Indeed, combination therapy has been shown by numerous studies to work synergistically, providing optimal and longer lasting clinical benefits than with either modality alone. Some clinicians consider combination therapy the standard for rejuvenation in the lower face.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


