Chapter 58 Pediatric dermatology
2. Name the papulopustular facial eruption often associated with inappropriate topical steroid use.
Periorificial dermatitis is a perioral, periorbital, and perinasal, erythematous, slightly scaling papulopustular eruption seen most commonly in preschool children. Treatment of this condition is the discontinuation of topical steroids and the use of the same oral or topical antibiotics that are used for acne vulgaris. Tetracycline and derivatives should not be used in children under 8 years of age.
6. Red, scaly, itchy, weight-bearing skin surfaces of the feet in children are usually not due to tinea pedis, but to what?
7. Plant dermatitis, such as poison ivy, is the most prevalent cause of allergic contact dermatitis in children. What are some others?
8. One- to 2-mm keratotic papules located on the face, outer upper arms, and thighs are frequently misdiagnosed as folliculitis. What are they really?
11. How is tinea capitis treated?
Oral griseofulvin is the treatment of choice. Oral terbinafine and itraconazole are also used. Topical antifungals have no role in the treatment of tinea capitis. Some authorities recommend twice-weekly shampooing with 2% selenium sulfide or ketoconazole shampoos as a useful adjunctive therapy to griseofulvin, because it is sporicidal and may prevent spread to other children and family members.

Trovato MJ, Schwartz RA, Janniger CK: Tinea capitis: current concepts in clinical practice, Cutis 77:93–99, 2006.
12. What is the hypersensitivity reaction to tinea capitis that is commonly mistaken for a bacterial superinfection?
14. What percentage of children with psoriasis will have guttate psoriasis?
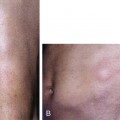
15. Describe the rash associated with childhood dermatomyositis.
A malar photosensitive rash, with red flat-topped papules on the knuckles (Gottron’s papules) and edematous plaques on the elbows and knees, is often seen in childhood dermatomyositis (Fig. 58-2). Unlike adult disease, childhood dermatomyositis is not related to internal malignancies.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


