10 Single and Multiple Levels with the PCM Cervical disk arthroplasty is a recently introduced option for patients otherwise undergoing anterior cervical diskectomy and fusion (ACDF) for nontraumatic indications. To the greatest extent possible in spine surgery, ACDF as a treatment for radicular and myelopathic symptoms represents a gold standard with long-term clinical experience, established indications, and reproducible clinical and surgical results.1 However, shortcomings of ACDF remain, including loss of segmental motion, possible adverse impacts upon adjacent segments,2 perioperative immobilization, bone graft site morbidity, pseudarthrosis with reoperation, and hardware failures. Because the incidences of the aforementioned are very low, any potential replacement treatment must meet a high standard. Cervical disk arthroplasty is a promising alternative, having been introduced as a means to allow motion preservation and potential avoidance or minimization of adjacent level degeneration while providing the requisite postdecompression height, stability, and alignment maintenance. Ideally, restoration of the normal kinematics of the lower cervical spine as outlined by White and Panjabi3 is the desired goal of cervical arthroplasty. To this end, total disk replacement arthroplasty has been reported to restore motion in the cervical spine.4 In general, the indications for anterior cervical disk arthroplasty are similar to the traditional indications for anterior cervical decompression (i.e., radiculopathy or myelopathy caused by either one or two levels of anterior cervical compression).5–9 Symptoms of arm weakness, paresthesia, and unremitting radicular pain with or without lower extremity hyperactive reflexes with documentation of a neural compressive lesion are generally accepted as requiring anterior cervical decompression. Following decompression, the surgical goals are the restoration of the intervertebral and neuroforaminal height to prevent recurrence of neurological compression. Cervical disk arthroplasty aims to achieve this restoration while maintaining the prevalence of motion in an ideally natural fashion. In some instances, for example, in patients with a congenitally narrow spinal canal and myelopathy, the maintenance of motion may be undesirable. This distinction has prompted the formation of specific cervical disk arthroplasty indications according to Pimenta et al and McAfee10,11 (Table 10–1). Inevitably, with experience, critical review of clinical outcomes, and the advancement of the technology and techniques, further clarification and stratification of indications for arthroplasty as opposed to fusion will be defined. Several criteria are to be considered in the design of devices for cervical disk arthroplasty.12 All device designs, like the PCM (Porous Coated Motion) Artificial Cervical Disc (Cervitech, Inc., Rockaway, NJ), pursue the following implant design and material–related objectives:
PCM (Porous Coated Motion)
Artificial Cervical Disc
 Indications for Cervical Arthroplasty
Indications for Cervical Arthroplasty
 The Design of the PCM (Porous Coated Motion) Artificial Cervical Disc
The Design of the PCM (Porous Coated Motion) Artificial Cervical Disc
 Evaluation of the Bone Ingrowth Characteristics in the Implant–Bone Interface Gaps
Evaluation of the Bone Ingrowth Characteristics in the Implant–Bone Interface Gaps
Indications for Cervical Arthroplasty
The Design of the PCM (Porous Coated Motion) Artificial Cervical Disc
 Maintenance of implant longevity and having predictable and physiologically tolerable wear properties
Maintenance of implant longevity and having predictable and physiologically tolerable wear properties
 Motion creating surfaces designed to permit motion in a physiologically desirable fashion
Motion creating surfaces designed to permit motion in a physiologically desirable fashion
 The ability to maintain position in the intervertebral space under the variety of anticipated loading situations
The ability to maintain position in the intervertebral space under the variety of anticipated loading situations
 Augmentation of the stability of the spinal segment
Augmentation of the stability of the spinal segment
 Clinical Study
Clinical Study Complications
Complications Conclusion
ConclusionClinical inclusion criteria | Patients 20 to 70 years old Degenerative disk disease with radicular or spinal cord compression |
Clinical exclusion criteria | Metabolic and bone disease Patients in terminal phase of chronic disease Patients with pyogenic infection or active granulomatosis Patients with neoplastic or traumatic disease of the cervical spine |
Indications for the press-fit (no screws) model | Radicular compression Herniation of the nucleus pulposus of C3–C4 to C7–T1 Anterior medullary compression Cervical spondylosis Nuclear magnetic resonance imaging evidence of mechanical compression of neural elements Nontraumatic segmental instability Neurological compression of one, two, three or four levels from C3–C4 to C7–T1 Primary degenerative disk disease Degenerative adjacent segment disease |
Indications for the flanged version (with screw fixation), in addition to the above | Suboptimal carpentry, understood as an irregular cut in the preparation of the vertebral end plate Anterior vertebral subluxation ≥ 3.5 mm Anatomical variation or previous surgery predisposing the segment to higher loads |
Contraindications to PCM disk arthroplasty | Ossification of the posterior longitudinal ligament Ankylosing spondylitis Spondylolisthesis with posterior element lesion Narrow cervical canal, anterior-posterior diameter < 10 mm Severe arthritis of the facet joints Overt instability or posterior column inadequacy |
The PCM implant is designed much like a joint surface replacement in that it provides an articulating surface between two end plates that bond to the adjacent vertebrae. Given the critical design parameters and the novel nature of cervical disk replacement, selection of familiar materials and design attributes were favored over those less proven or with less clinical experience. The biomaterials chosen, ultra high molecular weight polyethylene (UHMWPE) and cast cobalt-chromium-molybdenum (CoCrMo) alloy to form the articulating bearing surface, represent gold standard materials from the field of joint replacement. Compression-molded sheet polyethylene was preferred for its more favorable and predictable deformation properties versus the durable but brittle, highly cross-linked polyethylene. The end plate surfaces are coated with a titanium-calcium-phosphate (TiCaP) coating providing both a surface featuring 75 to 300μ pores and a biochemically favorable interface for bone ingrowth. Pioneered in the field of dental implants, this coating has been utilized by the lumbar SB Charité Artificial Disc (DePuy Spine, Raynham, MA) prostheses implanted outside of the United States since 1998, and very favorable bone ingrowth characteristics have been documented in animal studies.13 The resulting electrochemical contoured surface is also stronger than prostheses using plasma spray hydroxyapatite (HA) coating.
The cervical vertebral end plates are substantially rectangular in shape, with the highest bone density in the lateral and dorsal regions.14 Similarly the PCM implant end plate is greater in width than in depth, reflecting the desirability of a large surface area for maximum support and subsidence resistance.
Longitudinal rows of unidirectional ridges provide pullout resistance along the implant’s vertebral interface (Fig. 10–1), but with consideration given to the eventuality of implant revision, embedded fins or sharp projections were avoided, reducing the likelihood of either partial corpectomy or extensive bone grafting in a revision situation. Only the extent of bone resection typically employed for ACDF is needed for preparation of the PCM prosthesis, and excessive reaming or table-mounted fixation jigs are not utilized. Given reports of heterotopic ossification and “spontaneous” postoperative fusion across the vertebral levels, possibly enhanced by excess bone resection or reaming,15 end plate preservation is encouraged and incorporated in the implant design criteria. In the event that supplemental fixation to the “press-fit” is desired, a version of the prosthesis that is fixed with screws to the anterior surface of the vertebral body is available. These design variations are similar to those described for other cervical disk prostheses.16,17
Selection of the shape and curvature of the articulating surface is a critical design element in cervical disk replacement implant design. Based on anatomical reviews of the normal translational component present in cervical segmental motion and the location of the naturally occurring center of rotation, a large radius of curvature mimicking the normal cervical motion arc was selected (Fig. 10–2).
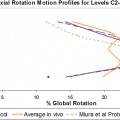
A comparison of ranges of motion of cadaveric spinal segments with intact, destabilized, fused, and both varieties of PCM cervical disk replacements confirmed the ability of the cervical disk replacement implants to maintain the motion properties of the intact spinal segment, versus the destabilized and fused segments8 (Fig. 10–3
Related posts:
 Prosthetic Disk Nucleus Partial Disk Replacement: Pathobiological and Biomechanical Rationale for Design and Function
Prosthetic Disk Nucleus Partial Disk Replacement: Pathobiological and Biomechanical Rationale for Design and Function
 Complications of Lumbar Disk Arthroplasty
Complications of Lumbar Disk Arthroplasty
 Spinal Kinetics Cervical Disc
Spinal Kinetics Cervical Disc
 Biomechanical Testing Protocol for Evaluating Disk Arthroplasty
Biomechanical Testing Protocol for Evaluating Disk Arthroplasty
 DIAM (Device for Intervertebral Assisted Motion) Spinal Stabilization System
DIAM (Device for Intervertebral Assisted Motion) Spinal Stabilization System
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


