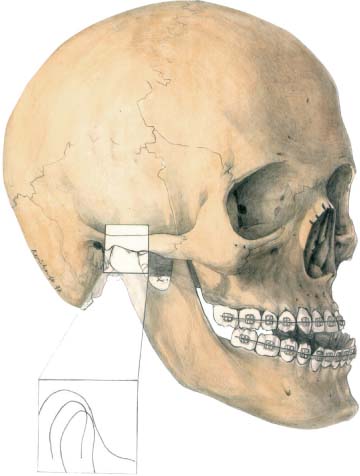
24 Orthognathic Surgery Distance Screws The simultaneous osteotomy of the maxilla and mandible, first described by Obwegeser in 1970, runs the risk of incorrect positioning of the maxilla, the mandible, and both condyles, if the opration is done without full supporting actions, including (but not limited to) an exact diagnosis, preoperative orthodontics, operation planning (method and simulation), and careful postoperative control. The use of miniplates and microplates in the midface and the mandible has led to greater convenience for patients; nevertheless, without the additional supporting activities referred to above the results will be dependent solely on the experience of the surgeon. Throughout the last quarter of the 20th century, significant developments in fields such as operation planning, operation simulation, and support skills and services have led to reproducible, lasting, and stable results from this operation. The double-splint method (Lindorf, 1977) is frequently used to control the horizontal dimension during the step-by-step positioning of maxilla and mandible in reaching a neutral occlusion. Controlling the vertical dimension is done intraoperatively by direct measurements between screwholesabove and belowthe Le FortIosteotomy line, or indirectly with extraoral appliances (Speculand and Jackson, 1984; Neubert, Bitter, and Somsiri, 1988; Luhr and Jäger, 1994), or intraorally using positioning plates (Wangerin, 1990). After preoperative orthognathic treatment, extensive clinical diagnosis, planning, and simulation of the operation are performed. First of all, the necessary clinical aesthetic parameters are considered and recorded, including the vertical facial symmetry that embraces the harmony of the three parts of the medial section of the face, the laugh line of the upper lip and the profile of the face. The stomatognathic system is evaluated, including the chewing function, tongue and mimic muscle activities, the condition of the teeth and the periodontium, and function of both temporomandibular joints. A panoramic radiograph is taken to judge the position of the mandibular canal and the wisdom teeth, where present. A lateral cephalogram is made for the Bergen analysis (Hasund, 1974), which provides information about maxillary and mandibular growth. In cases of asymmetries of the face a posterior–anterior cephalogram is necessary to determine the skeletal dimensions of abnormal jaw growth. These analyses are the basis for planning the operation. The unstable malocclusion leads to an undefined position of the condyles (Fig. 24.1). Therefore, a check bite in centric occlusion is performed to put the condyles in a physiological position (Fig. 24.2). These condylar positions are monitored radiographically while using the check bite. Plaster models of the maxilla and mandible are made to analyze the orthodontically aligned upper and lower dental arches. Cephalometric measurements on the lateral cephalogram determine the planned maxillary displacement. The aesthetic parameters are considered. The mandible is then placed in neutral occlusion to the maxilla. After analysis of the new facial profile a decision is made to determine the chin correction. The model of the maxilla is cut at the level of the Le Fort I osteotomy line. The model of the mandible is cut at the lower border of the mandible. By using the centric check bite, which is equivalent to the first splint, these separate models are arbitrarily mounted in an individual articulator system, for example, a SAM articulator, so that the yare level with an upper plane corresponding to the lower border of the mandible. Thus both jaws can be shifted in their proper planes. Subsequently the maxillary model is loosened from the upper plane and fixed with glue in the new position. The second splint is prepared in this relationship.
Introduction
Technique
Clinical Diagnosis
Radiographic Diagnosis
Model Diagnosis
Planning
Simulation
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


