Chapter 2 Optimizing Success in Aesthetic Breast Surgery
General Concepts
In many respects, quality breast surgery is as much a product of intelligent preoperative preparation and planning as it is sound technical skill. In fact, much of the most useful information that hopefully will come from this book will be contained in this chapter. As I have built my breast practice over the years, a pattern for success has emerged that has improved my personal results in both aesthetic and reconstructive breast surgery. This approach has made these results more consistent and helped tremendously in holding complications to a minimum. This approach can be divided into preoperative and intraoperative considerations.
Preoperative Considerations
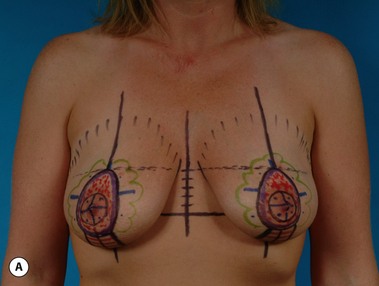
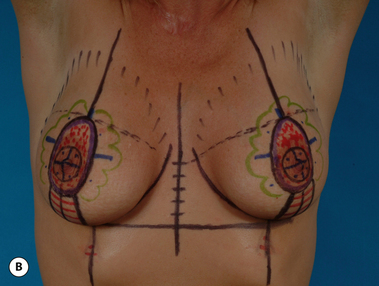
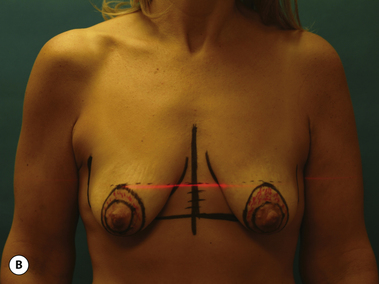
The second major goal of the preoperative visit is technical and relates to patient marking. As opposed to the often harried environment which is present in the hospital or surgical center, marking in the office allows the surgeon to apply all his or her energies to the task at hand in a quiet, controlled environment without interruption by anesthesia staff or nurses. All marking supplies will be readily available and experienced nursing staff assistance is assured. Marking done in conjunction with the administrative functions described previously assures that all issues will be addressed and greatly minimizes the potential for either significant or insignificant errors. Standard ‘permanent ink’ skin markers are used to identify pertinent landmarks as the patient stands upright in a relaxed position. Various multicolored packs of markers are available, with my personal preference being the ‘Sharpie’ brand, which offers up to 24 different colors (Figure 2.1). Bedsides the standard black and red, various other colors can be used to signify the particular surgical steps to be undertaken. For instance, areas of skin to be resected can be designated one color and areas where undermining is to be performed can be outlined in another. Any color scheme is appropriate and when this scheme is applied uniformly from patient to patient, the accuracy of the preoperative plan becomes enhanced. Essentially, the entire operative sequence is performed in the surgeon’s mind’s eye during the marking procedure with the marks documenting the surgical steps. In my opinion, the more detailed the marking pattern, the better the likelihood the proposed surgical procedure will be successful (Figure 2.2 A,B). One additional device which is quite useful is a standard laser leveler, which is available at most hardware stores. By dimming the lights and using the red laser light to reveal the true horizontal plane across the chest, accurate placement of important breast landmarks such as the top of the areola can be assured. Using this device can be very helpful, particularly in patients with preoperative asymmetries, where landmarks can be sometimes difficult to identify correctly and symmetrically (Figure 2.3 A,B).


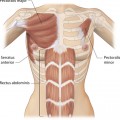
At this point, it is very important to note the patient’s natural shoulder position. Many patients will have an asymmetry in their shoulder level, which affects the position of the breast when the shoulder is artificially raised or lowered (Figure 2.4





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


