Chapter 5 Open Retromuscular Ventral Hernia Repair 
1 Clinical Anatomy
 Retrorectus repair requires a thorough knowledge of the relative anatomy of the myofascial components of the abdominal wall.
Retrorectus repair requires a thorough knowledge of the relative anatomy of the myofascial components of the abdominal wall.




 The lateral abdominal wall consists of three flat muscles: external oblique, internal oblique, and transversus abdominis. The flat muscles cross each other similar to a three-ply corset that strengthens the abdominal wall and diminishes the risk of herniation between the muscle bundles. One important consideration for the retrorectus repair is the fact that in the upper third of the abdomen, the transversus abdominis extends medially beyond the overlying linea semilunaris as a primary muscular component not as fascia (Fig. 5-1).
The lateral abdominal wall consists of three flat muscles: external oblique, internal oblique, and transversus abdominis. The flat muscles cross each other similar to a three-ply corset that strengthens the abdominal wall and diminishes the risk of herniation between the muscle bundles. One important consideration for the retrorectus repair is the fact that in the upper third of the abdomen, the transversus abdominis extends medially beyond the overlying linea semilunaris as a primary muscular component not as fascia (Fig. 5-1).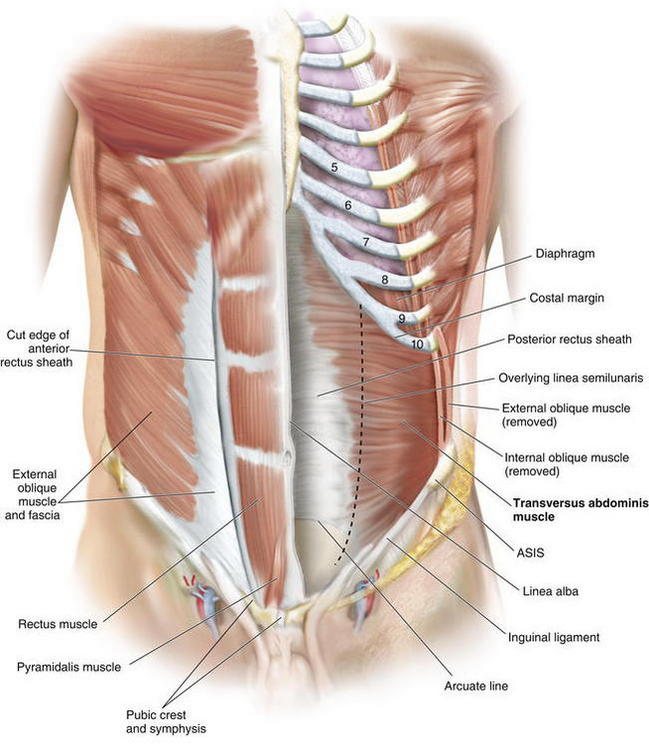
2 Preoperative Considerations
 Preoperative Imaging
Preoperative Imaging
 I recommend routine abdominal/pelvic computed tomography (CT) imaging. CT delineates all abdominal wall defects, assessment of the integrity of the remaining abdominal wall musculature, allows for detection of previous synthetic meshes and/or occult infection, and facilitates perioperative planning. I also mandate a screening colonoscopy in appropriate patients before undertaking major abdominal wall reconstructions.
I recommend routine abdominal/pelvic computed tomography (CT) imaging. CT delineates all abdominal wall defects, assessment of the integrity of the remaining abdominal wall musculature, allows for detection of previous synthetic meshes and/or occult infection, and facilitates perioperative planning. I also mandate a screening colonoscopy in appropriate patients before undertaking major abdominal wall reconstructions. Preoperative Optimization
Preoperative Optimization
 Nutritional evaluation and counseling for obese patients is paramount, and weight loss surgery should be considered.
Nutritional evaluation and counseling for obese patients is paramount, and weight loss surgery should be considered.





3 Operative Steps




 Lysis of Adhesions, Removal of Old Mesh
Lysis of Adhesions, Removal of Old Mesh
 Complete lysis of all visceral adhesions to the anterior abdominal and pelvic walls is performed. This is particularly important in cases where dissection lateral to the linea semilunaris is undertaken. Inter-loop adhesions are typically ignored.
Complete lysis of all visceral adhesions to the anterior abdominal and pelvic walls is performed. This is particularly important in cases where dissection lateral to the linea semilunaris is undertaken. Inter-loop adhesions are typically ignored.
 Incision of the Posterior Rectus Sheath (Rives-Stoppa-Wantz Technique)
Incision of the Posterior Rectus Sheath (Rives-Stoppa-Wantz Technique)
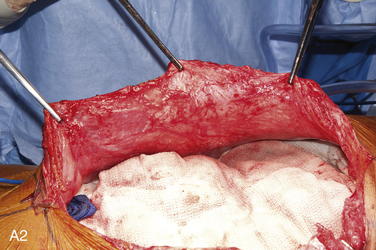
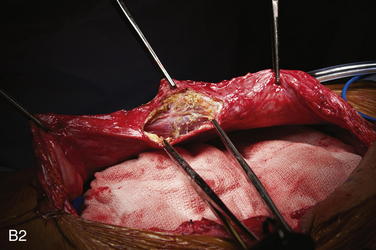
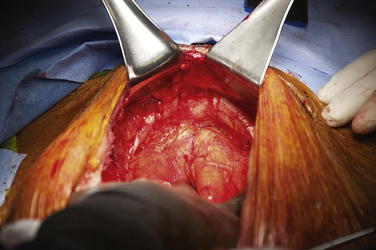
 To dissect the retromuscular space to the linea semilunaris, the posterior rectus sheath is incised sharply about 0.5 cm from its edge (Fig. 5-2, A). This typically is initiated at the level of the umbilicus. The retromuscular plane is then developed using a combination of blunt dissection and electrocautery. The lateral extent of this dissection is the linea semilunaris, confirmed by visualizing the junction between the posterior and anterior rectus sheaths (Fig. 5-2, B). Careful identification of the intercostal nerves and vessels is critical to maintaining an innervated functional abdominal wall (Fig. 5-2, C).
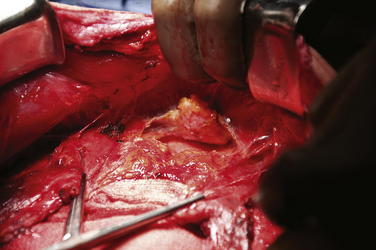
To dissect the retromuscular space to the linea semilunaris, the posterior rectus sheath is incised sharply about 0.5 cm from its edge (Fig. 5-2, A). This typically is initiated at the level of the umbilicus. The retromuscular plane is then developed using a combination of blunt dissection and electrocautery. The lateral extent of this dissection is the linea semilunaris, confirmed by visualizing the junction between the posterior and anterior rectus sheaths (Fig. 5-2, B). Careful identification of the intercostal nerves and vessels is critical to maintaining an innervated functional abdominal wall (Fig. 5-2, C). Exposure of Cooper’s ligaments/pubis is shown in Figure 5-3. Inferiorly, the space or Retzius is entered to expose the pubis symphysis and both Cooper’s ligaments. This dissection is blunt in what is typically a bloodless plane. Since this area is below the arcuate line, posterior layer includes peritoneum and transversalis fascia only. Because both of these layers are very thin, fenestrations are not uncommon and should be repaired. Care should be taken to identify and preserve inferior epigastric vessels that course along the deep surface of the rectus muscles. The urinary bladder may be filled with saline to facilitate its identification and dissection. This is particularly prudent in patients with a previous history of pelvic surgery.
Exposure of Cooper’s ligaments/pubis is shown in Figure 5-3. Inferiorly, the space or Retzius is entered to expose the pubis symphysis and both Cooper’s ligaments. This dissection is blunt in what is typically a bloodless plane. Since this area is below the arcuate line, posterior layer includes peritoneum and transversalis fascia only. Because both of these layers are very thin, fenestrations are not uncommon and should be repaired. Care should be taken to identify and preserve inferior epigastric vessels that course along the deep surface of the rectus muscles. The urinary bladder may be filled with saline to facilitate its identification and dissection. This is particularly prudent in patients with a previous history of pelvic surgery. Exposure of the subxiphoid space is shown in Figure 5-4. The retromuscular plane can be extended cephalad to the costal margin and to the retroxiphoid/retrosternal areas.
Exposure of the subxiphoid space is shown in Figure 5-4. The retromuscular plane can be extended cephalad to the costal margin and to the retroxiphoid/retrosternal areas.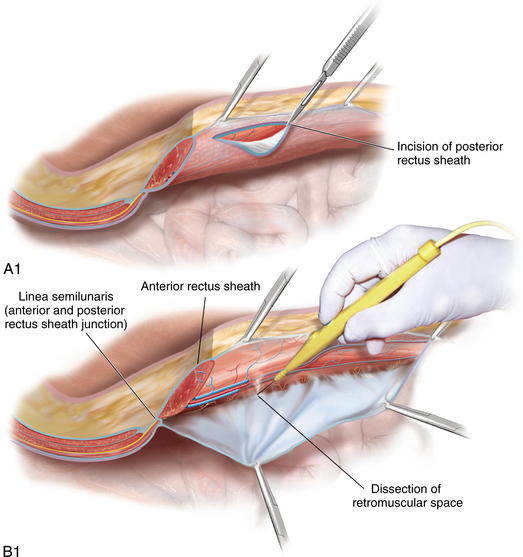

 Lateralization of the Dissection Plane Beyond the Linea Semilunaris
Lateralization of the Dissection Plane Beyond the Linea Semilunaris
 Traditional Rives-Stoppa-Wantz dissection is carried out to the lateral edge of the rectus sheath. However, such dissection is insufficient for some patients undergoing major abdominal wall reconstructions for three main reasons: (1) insufficient medial advancement of the posterior rectus sheath, (2) decreased potential for medialization of the rectus muscles, and (3) insufficient space for large prosthetic reinforcement.
Traditional Rives-Stoppa-Wantz dissection is carried out to the lateral edge of the rectus sheath. However, such dissection is insufficient for some patients undergoing major abdominal wall reconstructions for three main reasons: (1) insufficient medial advancement of the posterior rectus sheath, (2) decreased potential for medialization of the rectus muscles, and (3) insufficient space for large prosthetic reinforcement.Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


