Chapter 7 Open Repair of Parastomal Hernias 

2 Clinical Anatomy
1 Dissection Planes
 Abdominal wall anatomy is discussed in detail in Chapter 1. It is essential to understand the anatomic layering of the abdominal wall for proper retrorectus/retroperitoneal mesh placement and anterior component separation.
Abdominal wall anatomy is discussed in detail in Chapter 1. It is essential to understand the anatomic layering of the abdominal wall for proper retrorectus/retroperitoneal mesh placement and anterior component separation.
 Anterior component separation involves division of the external oblique aponeurosis lateral to the rectus sheath. Access for this division can be achieved via subcutaneous flap or via laparoscopic techniques as described previously (see Chapters 8 and 11) (Fig. 7-1).
Anterior component separation involves division of the external oblique aponeurosis lateral to the rectus sheath. Access for this division can be achieved via subcutaneous flap or via laparoscopic techniques as described previously (see Chapters 8 and 11) (Fig. 7-1).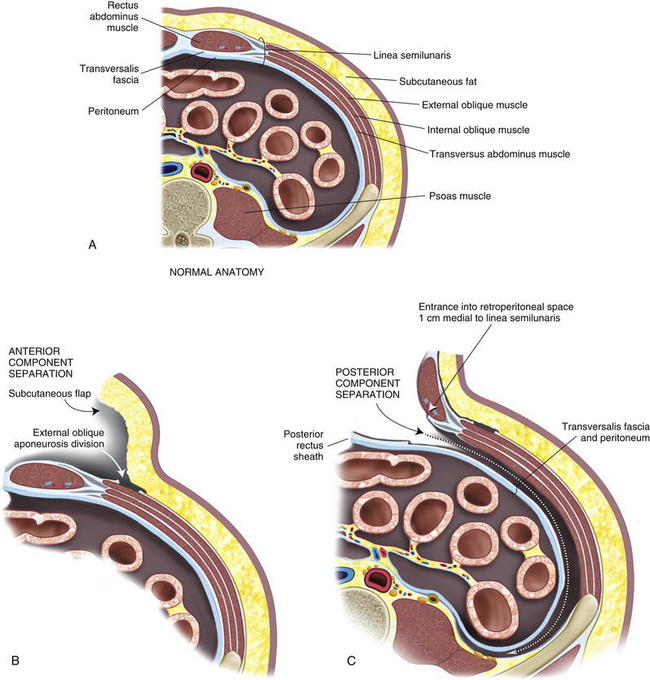
2 Ostomy Site Selection
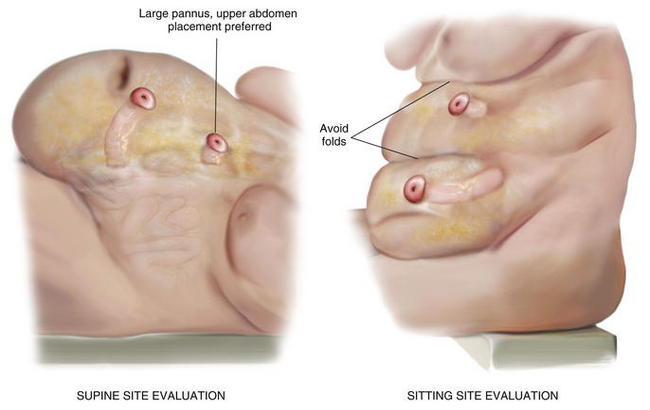
 Ostomy sites are chosen with the assistance of an enterostomal therapist and are marked preoperatively. Patients should be examined while sitting and supine, and an appropriate location visible to the patient is found. Transrectus placement is typically preferred. Folds should be avoided to facilitate appliance adhesion. Thus, it is essential to examine the patient while he or she is sitting in order to visualize folds. Obese patients with a significant pannus should be sited in the upper abdomen. During complex abdominal wall reconstruction, excess skin and subcutaneous tissues are often resected, and therefore consideration must be given to the eventual placement of the stoma (Figs. 7-2 and 7-3).
Ostomy sites are chosen with the assistance of an enterostomal therapist and are marked preoperatively. Patients should be examined while sitting and supine, and an appropriate location visible to the patient is found. Transrectus placement is typically preferred. Folds should be avoided to facilitate appliance adhesion. Thus, it is essential to examine the patient while he or she is sitting in order to visualize folds. Obese patients with a significant pannus should be sited in the upper abdomen. During complex abdominal wall reconstruction, excess skin and subcutaneous tissues are often resected, and therefore consideration must be given to the eventual placement of the stoma (Figs. 7-2 and 7-3).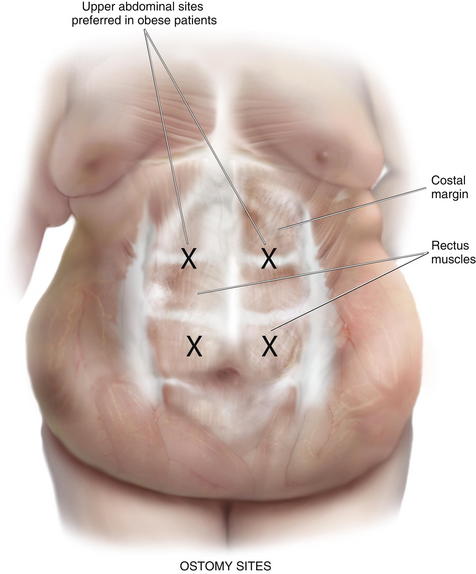
3 Preoperative Considerations
1 Comorbidities
 Appropriate patient selection and optimization is essential. The procedure results in a significant physiologic insult. An extended operation with a long midline incision and prolonged adhesiolysis is typical. Significant fluid shifts should be expected. Those with extensive cardiac, pulmonary, or renal disease should be vetted carefully and optimized maximally. Risk of surgery may be prohibitive in some.
Appropriate patient selection and optimization is essential. The procedure results in a significant physiologic insult. An extended operation with a long midline incision and prolonged adhesiolysis is typical. Significant fluid shifts should be expected. Those with extensive cardiac, pulmonary, or renal disease should be vetted carefully and optimized maximally. Risk of surgery may be prohibitive in some.



2 Two-Team Approach
 We have found a two-team approach particularly efficacious. One team focuses on adhesiolysis, intestinal mobilization, resection, and repair as appropriate. A second team proceeds with abdominal wall reconstruction. In our institution, we typically use a colorectal surgical team and a general surgical team. Although, one surgeon can certainly accomplish these procedures, fatigue of the operating team does become a factor with operative times averaging about 5 hours. A planned two-team approach helps facilitate procedure progression in these prolonged cases.
We have found a two-team approach particularly efficacious. One team focuses on adhesiolysis, intestinal mobilization, resection, and repair as appropriate. A second team proceeds with abdominal wall reconstruction. In our institution, we typically use a colorectal surgical team and a general surgical team. Although, one surgeon can certainly accomplish these procedures, fatigue of the operating team does become a factor with operative times averaging about 5 hours. A planned two-team approach helps facilitate procedure progression in these prolonged cases.





