Chapter 9
EVALUATION OF THE LACRIMAL SYSTEM
John L. Wobig and Roger A. Dailey
Approximately 30% of the patients who visit an ophthalmologist have lacrimal problems. Of these patients, perhaps half have symptoms that involve only the secretory system. Especially among the elderly, the constant complaint is “burning, smarting, tearing” eyes. The harried ophthalmologist often does not take the time to do a 5-minute Schirmer No. 1 test, and gives the patient any one of a dozen different samples of “artificial tears.”
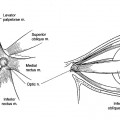
The anatomy of the secretors has been previously discussed. The secretory tests should be repeated two or more times on different days to get a reliable average. The variability from one day to another in lacrimal hyposecretion often is due to pseudoepiphora one day followed by a fatigue block the next. This can be discovered only by using the basic secretion and Schirmer No. 2 tests.
SECRETORY DIAGNOSTIC TESTS
The basic secretion test will differentiate between basic secretion and reflex secretion. The Schirmer No. 2 test will reveal fatigue block. These tests help eliminate some of the variability in testing for hyposecretion (Fig. 9-1).
SCHIRMER NO. 1 TEST
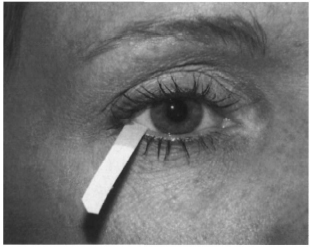
This test is used to differentiate hyposecretion and psuedoepiphora from normal secretion (see Chapter 10 for description of hyposecretion) (Fig. 9-2). The room should be moderately lighted and the patient should face away from any direct light.
A piece of Whatman No. 41 filter paper (S.M.P. Division of Cooper Laboratories, Inc., San German, Puerto Rico), 5 mm wide x 35 mm long, is partially folded 5 mm from one end. The folded short end is placed on the lateral one-third of the lower tarsal conjunctiva and the patient is asked to fix both eyes on any object slightly above the direct line of gaze for 5 minutes.
If the wetting is between 10 and 30 mm, it may be normal or may denote pseudoepiphora, in which the reflex secretors are compensating for decreased basic secretion. Wetting > 30 mm usually has no differential value; the patient may have pseudoepiphora, hypersecretion, or normal secretion. Wetting < 10 mm is hyposecretion.
BASIC SECRETION TEST
The basic secretion test is used to differentiate basic secretion from reflex secretion. In normal eyes, this test should be done in a dark room. When some degree of hyposecretion is apparent, however, it may be done in a moderately lighted room, as in the Schirmer No. 1 test.
Two or more drops of a local ophthalmic anesthetic are instilled in the conjunctival sac of both eyelids. After waiting for 1 or more minutes for topical anesthesia to occur and for any hyperemic reaction to subside, the lower cul-de-sac is gently dried with a cotton-tipped applicator and a second applicator, moistened with cocaine hydrochloride (5%) with adrenalin chloride (1:1,000), is applied to the conjunctiva for about 1 minute to obtain deeper anesthesia where the filter paper will rest. If < 10 mm of wetting occurs in 5 minutes, hyposecretion due to failure of the basic secretors alone is present (if the patient feels the filter paper, the test is of no value).
When this test follows a diagnosis of hyposecretion by the Schirmer No. 1 test, the difference between the two readings denotes the amount of fluid contributed by the reflex secretors. When the Schirmer No. 1 test has shown > 10 mm of wetting, it denotes the effort of the reflex secretors to compensate for failure of the basic secretors (pseudoepiphora).
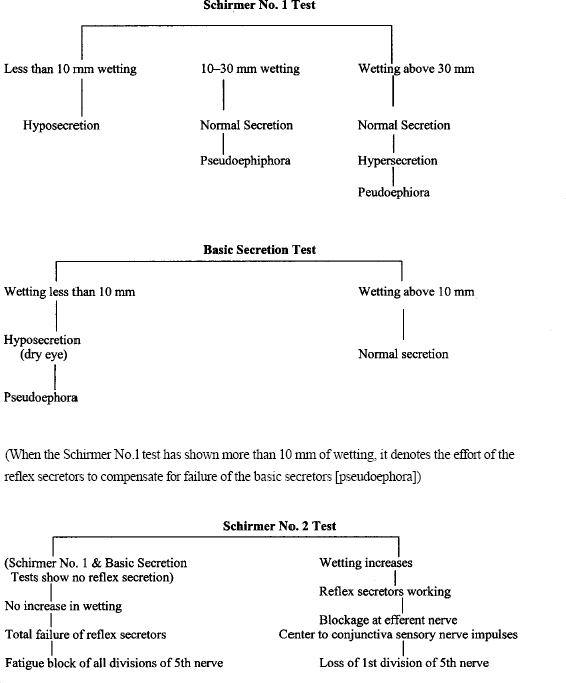
FIGURE 9-1 Secretory flow Charts.
SCHIRMER NO. 2 TEST
When the Schirmer No. 1 test or the basic secretion test shows that there is no reflex secretion, the Schirmer No. 2 test is used to find out whether the reflex secretors are gone or that only a “fatigue block” is present.
The conjunctiva of one eye is anesthetized. Filter paper is inserted inside the eyelid and the unanesthetized nasal mucosa in the region of the middle turbinate is irritated by rubbing it with a fairly large, dry, cotton-tipped applicator. The amount of wetting is tabulated after 2 minutes.
There is, at present, no objective test for psychogenic reflex tearing. However, patients with a proved decrease in or absence of reflex secretion due to a fatigue block of the peripheral sensory impulses will give a history of copious tearing during emotional stress. Reflex tearing is often the result of a combination of peripheral sensory and psychogenic stimulation.
Classification of secretory conditions is as follows:
1. Hypersecretion
a. Diagnosis: Complaint of tearing, evidence of above average Schirmer No. 1, normal excretory system, normal distributional system
b. Treatment: Closure of ducts between main and accessory glands, and conjunctival dacryocystorhinostomy
2. Hyposecretion
a. Diagnosis: Schirmer No. 1 < 10 mm, rapid breakup time
b. Treatment: Occlude punctum
3. Pseudoepiphora
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


