9 Not too Tight: Skin Tightening Procedures
Summary
In recent years, the popularity of cosmetic procedures has continued to rise, including those that serve to treat fine lines and wrinkles and skin laxity. Traditionally, women have comprised the vast majority of patients. However, men now represent a growing portion of patients. Due to several important differences in anatomy, perspectives, and preferences, the treatment approach to skin tightening should be tailored to men when treating this particular group. Practitioners should be knowledgeable about the various types of treatment that are available and understand the unique approach in order to continue to deliver effective, tailored, and high-quality care.
Keywords: aesthetics skin tightening lasers ultrasound therapy radiofrequency microneedling wrinkles
9.1 Background
Over the past decade, the field of aesthetics has witnessed remarkable growth. What had originally started as a small subspecialty built around injectable neuromodulators and soft-tissue fillers has now grown to encompass numerous lasers and medical devices utilizing various technologies. According to the American Society for Dermatologic Surgery (ASDS), members performed more than 12.5 million procedures in 2018 alone, which was 7.8 million in 2012.1 The top procedures were skin cancer treatments, injectable neuromodulators and soft-tissue fillers, and laser-, light-, or energy-based procedures. In the past 7 years, there was a 78% increase in soft-tissue filler treatments, a 74% increase in laser-, light-, or energy-based procedures, and a nearly 400% increase in body contouring procedures.1 The numbers continue to grow each year as new devices and technologies are brought to the aesthetic market. The reasons why people are turning to cosmetics to enhance their appearance is well apparent in the ASDS survey data (Fig. 9.1).
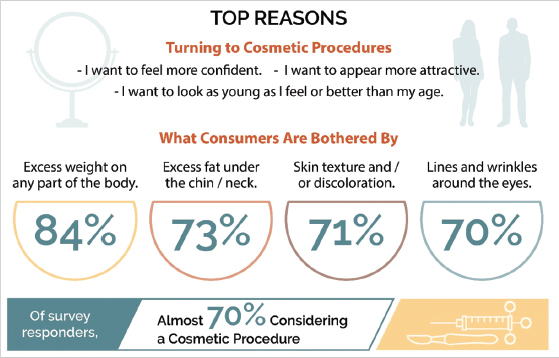
Fig. 9.1 Key factors behind the increase in cosmetic procedures. (Reproduced with permission from the American Society for Dermatologic Surgery: 2019 Annual Consumer Survey on Dermatologic Procedures.)
While part of this growth is due to the more recent expansion of technology coupled with the innovation of newer medical devices, consumer-driven growth has continued to play an ever-expanding role. With the rise of social media platforms, networking websites, and mobile applications, consumers and patients are more connected to each other than ever before. The trend to take and easily transmit mobile phone camera photographs of one’s self has fostered a social “sharing” of images centered on one’s physical attributes. Especially with many mobile and computer applications that can “filter” or alter one’s appearance in either subtle or substantial ways, the new reality is that the current technology has significantly changed the perception of beauty worldwide.2,3,4
Whereas the population of patients seeking cosmetic treatments has traditionally been predominately female, a growing number of men are now looking to have aesthetic procedures done. Due to the rapidly expanding market of male aesthetics, it is important for clinicians to understand the available treatment options, including skin tightening procedures (Fig. 9.2). Despite more men doing aesthetic procedures, there still continues to be barriers in place for men. There tends to be a lack of acceptance or stigma of doing cosmetic procedures among peers, more so for men than women. Also, there tends to be a general lack of knowledge of what can be done for men that will not make them look unnatural or feminine. Due to anatomical differences, specifically increased skin thickness and collagen density, facial aging in general is often less noticeable in men than in women.5–7 However, males begin to experience decreases in skin thickness earlier on in their 20 s. Furthermore, a greater degree of muscle movement with facial expressions compared to women has been thought to contribute to deeper wrinkles.8,9 Due to the rapidly expanding market of male aesthetics, it is important for clinicians to understand the available treatment options, including skin tightening procedures as a noninvasive option for men.
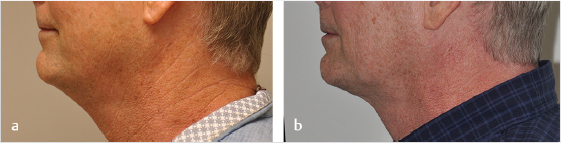
Fig. 9.2 (a) Before and (b) five months after single session of ThermiTight(R). (Courtesy of Jason D. Bloom, MD, FACS [Facial Plastic Surgeon].)
Cutaneous aging and skin laxity can be quite striking in both genders. Along with intrinsic aging, facial skin is particularly vulnerable to environmental stressors that patients are exposed to on a regular basis, such as ultraviolet radiation, smoke, and pollution. It has also been demonstrated that severe solar elastosis of the head and neck region was more common in men than in women.10 These environmental insults can each lead to cellular stress and subsequent injury, where repetitive exposures can cause an accumulation of damage that can be harmful to cellular function, protein maturation, and normal skin physiology.11,12,13,14 The skin’s natural elasticity and firmness can be lost due to the resultant breakdown of collagen and elastin in addition to a reduction in fibroblast activity. Collagen types I and III represent approximately 75% of the dry weight of the dermis and 20 to 30% of its volume.15 Fibroblasts generate new collagen, whereas matrix metalloproteinases (MMPs) degrade it, typically maintaining a balance. Ultraviolet radiation and other intrinsic and extrinsic sources of reactive oxygen species upregulate the production of MMPs, resulting in accelerated skin aging.16 Elastin comprises 4% of the dry weight of the dermis and gives the skin its mechanical strength and ability to resist deformation, or elasticity.17 Intrinsic aging causes atrophy of elastin fibers, whereas extrinsic aging, such as ultraviolet light exposure, causes a disorganization in the elastic fiber network resulting in solar elastosis.18 The vital role of elastin in maintaining the structure of the extracellular matrix is well established; even the slightest decrease in the number of elastin fibers results in significant changes in skin elasticity and strength.
Clinically, these cellular and chemical effects can cause the familiar signs of cutaneous aging that people are accustomed to seeing, such as fine lines and wrinkles, thinning, roughness, dyspigmentation, coarseness, and decreased elasticity. Since skin laxity is a common cosmetic complaint of those seeking consultations, physicians should be familiar with recognizing and treating this condition.
9.2 Indications
The gold standard for correcting skin laxity and achieving tightening is surgical correction, such as rhytidectomy. Although consistently and uniformly effective, surgical procedures can be invasive, risky, costly, and inappropriate for some patients. As such, the demand for less invasive treatment modalities has increased. Minimally invasive skin tightening devices, when utilized correctly, can be effective in treating skin laxity. An individual modality may be more fitting to a specific patient depending on the clinical grade, depth, and degree of the laxity in addition to the preference for concurrent resurfacing and desired outcomes. An individualized treatment plan is always recommended in order to achieve ideal clinical outcomes as opposed to a one-size-fits-all approach in aesthetics.
9.3 Patient Selection
The importance of patient selection cannot be emphasized enough, especially since it represents a critical part for determining adequate clinical outcomes and patient satisfaction. When selecting patients for treatments of skin laxity using minimally invasive methods, it is best for patients to have mild to moderate skin laxity. Too significant or severe skin laxity may be more suitable for an invasive or surgical approach, such as a rhytidectomy (facelift), which may offer better outcomes.
In addition to proper patient selection, the management of expectations is equally as important. Minimally invasive modalities can be effective, but only in the right clinical scenario. It is crucial to advise patients of the limitations of skin tightening procedures that utilize medical devices, especially when compared to surgical options in patients with significant skin laxity. Less than ideal outcomes would be the rule rather than the exception in some scenarios involving severe laxity, and postprocedural results may not adequately satisfy the patient. Sufficiently addressing patient expectations is vital to ensure a high level of patient satisfaction and subsequent patient retention. Men are often less inclined to undergo large surgical operations from plastic surgeons and may prefer decreased postprocedural downtime often due to work commitments.
Prior to any procedures and ideally during the visit for aesthetic consultation, multiple photographs should be taken. Photographs from various angles using appropriate, standardized lighting are recommended. These photographs can help demonstrate the level of skin laxity to patients prior to any treatments being completed and can also be used to grade treatment effects for comparison. Although clinical scales for skin laxity have been developed, they are neither universally used nor specific for male patients.19,20 Occasionally, patients may believe that treatments have not resulted in clinical improvements, in which case, these photographs can be of immense benefit to the practitioner.
9.4 Treatment Options
9.4.1 Microneedling
Microneedling, known as percutaneous collagen induction (PCI) therapy, has been utilized to treat a variety of cutaneous conditions, including skin laxity.21,22 Extremely small needles are used to pierce the epidermal and dermal layers to create columns of physical injury. The depth of penetration can be selected depending on the condition and site, which can also be layered to create larger areas of controlled injury. After the damaged collagen is removed, new synthesis and remodeling subsequently occur, which are supported by the stimulation of various growth factors and fibroblasts.23 A recent study showed significant improvements in global wrinkle score, skin laxity, and skin texture at 150 days following a series of four microneedling treatments in 48 subjects.24 Although the results from microneedling can be modest, it represents an inexpensive modality that can concurrently treat the epidermis. Whereas these devices are primarily used for improving skin texture, treating minimal skin laxity may also be possible. The depths of needle penetration may offer improved results when increased for males with thicker skin, especially on the cheeks.
Whereas traditional devices initially came in the form of manual rollers, newer automated devices such as pens are now more commonly utilized.25 The newer pens allow for rapid adjustments of depth and frequency in addition to the hygienic use of disposable, single-use tips. A thin layer of gliding solution is recommended at faster speeds to allow for easy movement without “catching” of the skin. Automated pens should be held perpendicular, and multiple passes in different directions are recommended. For microneedling, the treatment endpoint is typically transient pinpoint bleeding.
Ablative and Nonablative Lasers
Ablative resurfacing lasers represent the traditional gold standard for the treatment of facial rejuvenation and skin laxity. By targeting water in the skin for vaporization, lax skin can be selectively targeted for removal. Due to complete epithelial destruction, new collagen formation occurs after the prolonged downtime that is required for full re-epithelialization. Treatments are associated with increased risks of adverse events, such as dyspigmentation and scarring. Compared to newer modalities, treatments are limited to superficial depths.
The introduction of nonablative lasers was met with both greater acceptance and increased demand due to its decreased postprocedural downtime when compared to their ablative counterparts. Adverse events are also more limited. The thermal energy can reach and bulk heat the dermis to induce physiologic changes as described earlier, while sparing the overlying epidermis with concurrent superficial cooling. Although better tolerated than the ablative lasers, clinical outcomes are more modest due to less thermal injury being delivered.
In 2004, fractional photothermolysis was introduced, which resulted in a paradigm shift in aesthetic treatment options.26 In contrast to treating the entire skin, only portions are treated by using thermal injury to create small columns, termed microscopic treatment zones (MTZs). Their density, width, and depth can be controlled by the practitioner. Male patients may tolerate greater densities if required. Since these damaged columns are surrounded by untreated and unaffected skin, the duration of postprocedural downtime is significantly decreased because these act as healing reservoirs. Ablative fractional resurfacing may also be superior to its traditional counterpart for treating skin laxity, since it has the ability to penetrate deeper into the dermis.27 As with nonfractionated devices, ablative modalities still offer improved clinical outcomes compared to nonablative devices. Confluent and fractionally ablative modalities can also be combined safely to offer effective results.28 Due to limited depths, ablative and nonablative lasers are more suited to treat mild skin laxity or if other epidermal skin conditions are simultaneously being treated.
9.4.2 Radiofrequency
Radiofrequency (RF) has been used as a method to cause controlled dermal heating for purposes of skin tightening since 2001.29 Instead of harnessing the power of light, RF uses an electric current to deliver energy to the dermis for thermal collagen remodeling.30 Heat is generated from the tissue resistance to the movement of electrons within the RF field to typically heat the area between 43 and 45 °C, whereas the epidermis is cooled. The depth of penetration is inversely proportional to the frequency. The mechanisms by which RF devices produce skin tightening are volumetric heating of the dermal structures, such as collagen and fascia, and induction of a wound healing response. An earlier study in 2003 demonstrated the safety and efficacy of a single RF treatment for periorbital skin laxity in 86 patients, which included several objective and subjective measures.31 In addition to clinical improvements, electron microscopy has also evidenced thicker collagen fibers associated with treatments.32
Numerous devices deliver RF energy in various modes, including unipolar, monopolar, bipolar, and multipolar. Unipolar RF is difficult to control with greater chance to cause deeper tissue damage, whereas multipolar RF can deliver more uniform wavelength penetration.33 Monopolar RF typically utilizes a grounding plate, where the energy is driven deeper down through the skin’s layers and structures. Monopolar energy can be delivered in a stamped mode, gliding movement, or subcutaneous fiber, and recent analyses have demonstrated monopolar RF’s seemingly effective and safe treatments.34,35 In comparison, bipolar and multipolar RFs deliver the energy between the poles of the handpiece, and the depth of penetration is controlled by the distance between them. Bipolar and multipolar devices do not deliver RF energy as deep, since the current has a controlled distribution that is limited to the volume between the electrodes.36 For this reason, they have been suggested to be more helpful for either younger patients who desire prevention or those with mild laxity.37 Newer devices are equipped with subdermal probes and real-time monitoring to increase patient safety and reduce the potential for overheating, which can cause unintended burns, local damage, blistering, necrosis, and scarring. RF devices can typically cause deeper effects than the previously mentioned modalities. Male patients with greater laxity may benefit from monopolar RF due to deeper penetration.
9.4.3 Radiofrequency Microneedling
The concept of fractionation has classically been applied to lasers, particularly resurfacing lasers, such as the carbon dioxide laser. However, fractionation has also been applied to RF as well. In recent years, RF has been combined with traditional microneedling, termed “RF microneedling.” This is by definition, a fractional treatment. The device utilizes a small needle array to penetrate the epidermal and dermal layers and deliver RF energy through the needles to the dermis.25,38 Physicians can choose to use either insulated or noninsulated needles. Insulated needles deliver energy focused at the tips of the needles, whereas noninsulated needles deliver RF energy from a larger focus to cause more thermal injury. Tips can also be used in monopolar and bipolar modes, which control the flow of the RF energy. Noninsulated tips and monopolar modes are thought to deliver increased and deeper injury, but also with an increased risk of adverse events. Multiple delivery systems differ in needle length, needle coating, needle sharpness, and method of needle insertion. A recent study showed improvements in wrinkle reduction, skin tightening, and lifting of the mid to lower face using a noninsulated RF microneedling system in 49 patients undergoing 3 monthly treatments.39 Skin laxity, particularly of the lower face and neck, is an excellent indication for RF microneedling treatment.
The addition of RF energy can increase the amount and depth of controlled injury to the dermis compared to traditional microneedling. Treatments can be layered to create additional injury at various depths, which supports enhanced neocollagenesis and remodeling, above and beyond the trauma induced by microneedling alone. In contrast to traditional microneedling, no gliding solution is needed and pinpoint bleeding is not necessarily expected depending on the treatment parameters. The needles penetrate and retract instead of oscillating, so it is important to allow for full retraction before moving sites in order to prevent dragging and unintended thermal damage to the skin (Fig. 9.3).
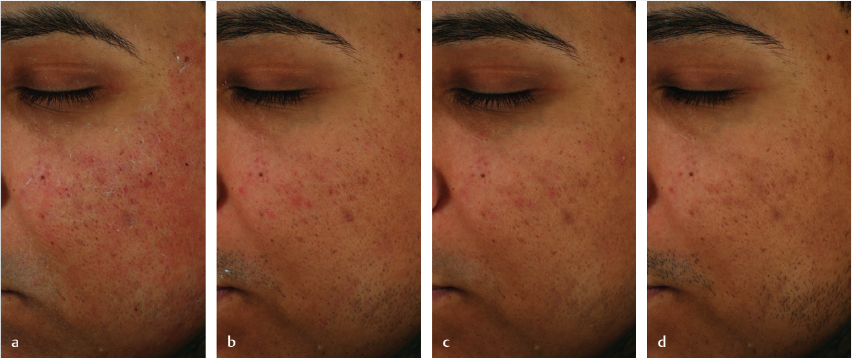
Fig. 9.3 Male patient following radiofrequency microneedling at (a) immediate post, (b) 2 days post, (c) 4 days post, and (d) 7 days post treatment demonstrating post-procedural downtime and healing. (Courtesy of Jordan V Wang, MD, MBE, MBA and Roy Geronemus, MD.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


