Fig. 39.1
(a, b) Preoperative view. A 44-year-old patient had a multicentric carcinoma in situ in both the upper quadrants of the left breast. The breast was of medium size with moderate ptosis
39.2 Surgery
Nipple-sparing mastectomy was done through a lateral incision. Nipple coring was performed and retroareolar frozen section biopsy revealed a tumor-free specimen. A subpectoral pocket was dissected with the pectoralis major muscle separated from its origins in the inframammary fold and medially to the height of the nipple position. A 370 cc anatomical implant was inserted and covered in the inferior pole with an acellar dermal matrix (ADM) which was fixed to the muscle and to the inframammary fold with a running suture (2.0 vicryl). One drain was placed in the subpectoral pocket and another one in the mastectomy pocket. Sentinel node biopsy found two negative sentinel nodes.
39.3 Clinical and Cosmetic Outcome
Final histology found a multicentric carcinoma in situ completely removed. The postoperative course was uneventful. No further treatment was suggested.
The postoperative result was rated as excellent by the patient and surgeon (Fig. 39.2a, b).
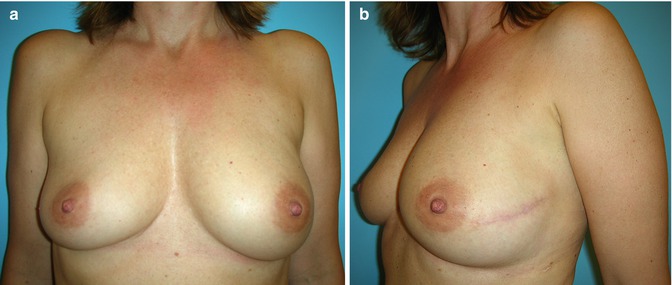
Fig. 39.2
(a, b) Postoperative view after nipple-sparing mastectomy and immediate reconstruction with an implant and a Strattice® ADM
39.4 Comments of Author
The location of the incision for mastectomy largely depends on the breast size, the ptosis, the location of the tumor, and the preference of the surgeon. Although a nipple-sparing mastectomy is oncologically safe, the pros and cons have to be discussed with the patient, and the preference of the patient for a skin-sparing mastectomy has to be respected (Fig. 39.3a–f). Preserving the nipple carries the risk of necrosis, and due to nipple coring, the nipple is completely numb.Get Clinical Tree app for offline access
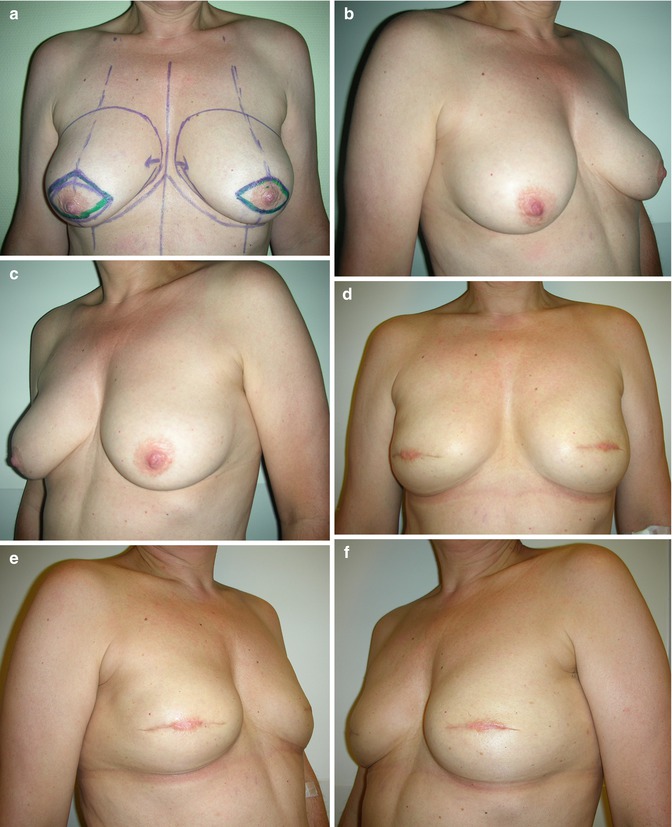
Fig. 39.3
(a–f) Pre (a–c)- and postoperative (d–fRelated posts:
 Doughnut Lumpectomy: Caveat II
Doughnut Lumpectomy: Caveat II
 Doughnut Lumpectomy: Caveat I
Doughnut Lumpectomy: Caveat I
 Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
 Defect Reconstruction After Breast Conservation Surgery and Radiation with Lipofilling
Defect Reconstruction After Breast Conservation Surgery and Radiation with Lipofilling
 Mastectomy and Immediate Expander Reconstruction for Local Breast Recurrence After Previous Quadrantectomy and Radiation
Mastectomy and Immediate Expander Reconstruction for Local Breast Recurrence After Previous Quadrantectomy and Radiation
 Immediate Implant-Based Breast Reconstruction with an Acellular Dermal Matrix (ADM): Reconstruction Failure Due to Postoperative Hematoma Causing Skin Necrosis and Implant Extrusion
Immediate Implant-Based Breast Reconstruction with an Acellular Dermal Matrix (ADM): Reconstruction Failure Due to Postoperative Hematoma Causing Skin Necrosis and Implant Extrusion

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


