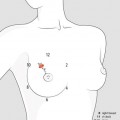
Fig. 10.1
Secretions should be obtained from the nipple by a centripetal, gentle pressure at the base of the areola
Fig. 10.2
The woman may help in locating area the pressure of which can cause the secretion
Nipple discharge is considered spontaneous when it occurs easily, without a persistent stimulation. It should be considered spontaneous even when the woman reports a history of bloody discharge and supports it with the finding of stains of blood on her bra or underclothing.
Grouping. Different appearances of mammary secretions should be gathered in three groups:
Milky or milky white (galactorrhoea), functional or idiopathic, of little significance
Coloured opalescent (non-galactorrhoea and non-bloody), usually more or less brown-stained but also lipidic or comedones (cheesy appearance) as an expression of ductal ectasia, also of little significance
Bloody or blood-related (serous, watery), the only really significant, especially if real, spontaneous, persistent and not related to breastfeeding
Milky and coloured opalescent secretions are physiologic in most of cases, while bloody or blood-related secretions are mostly pathologic. The main characteristics and clinical significance of the groups of nipple discharge are shown in Table 10.1.
Table 10.1
Characteristics and clinical significance of the groups of nipple discharge
Groups | Characteristics | Significance | |
|---|---|---|---|
Physiologic in most cases of little significance; require no treatment | Milky or milky white (galactorrhoea) | Slight galactorrhoea | Slight galactorrhoea is idiopathic in most cases |
True galactorrhoea | Only true galactorrhoea may be suggestive of prolactinoma | ||
Coloured opalescent (non-galactorrhoea and non-blood) | Fibrocystic changes | All appearances are the more or less extreme result of hormonal and/or involutional changes | |
Duct ectasia phenomena, from flawing to dense secretions | |||
Pathologic in most cases due to papillary lesions | Blood or blood–related (serous, watery) | Bloody or blood-stained | All appearances have the same significance with a high risk of papillary lesions (benign and malignant) |
Serous | |||
Watery |
MILKY (GALACTORRHOEA). It is crucial to distinguish slight galactorrhoea from true galactorrhoea.
Slight galactorrhoea. The discharge is milky or more often serous-milky whitish or colourless, poorly consistent, depending on the content of proteins (serum albumin, globulins and lactalbumin), but especially of lipids. Discharge is bilateral, at low profusion, easy but non-spontaneous, while prolactinaemia is normal or slightly increased.
The symptom may be secondary to a reduced antagonism of progesterone lactogenic action of prolactin in the presence of anovulatory cycles or luteal insufficiency. It occurs bilaterally after a pregnancy, but also in the course of hormonal therapy with neuroleptics, especially in the presence of a marked breast involution (fatty breasts). In approximately 20–25 % of women, slight galactorrhoea has not any evident reason and is probably due to a greater glandular receptivity to low levels of prolactin, so that it should be considered idiopathic.
Galactorrhoea, idiopathic or otherwise normoprolactinaemic, usually not bothersome, requires no action. Treatment of galactorrhoea secondary to thyroid or ovarian dysfunction should be, as far as possible, etiological. If neuroleptics or other drugs are responsible (Table 10.2) [2], in some (few) cases it could be necessary to correct or restrict their use.
Table 10.2
Medications that cause hyperprolactinaemia (effect may be dose-dependent)
Antipsychotics, first generation: chlorpromazine, loxapine, perphenazine, pimozide, thiothixene, trifluoperazine, ziprasidone (moderate); fluphenazine, haloperidol (high) |
Antipsychotics, second generation: aripiprazole, clozapine, iloperidone, lurasidone, olanzapine, quetiapine (none or low); asenapine (moderate); paliperidone, risperidone (high) |
Antidepressants, tricyclic: nortriptyline (none); amitriptyline, desipramine (low); clomipramine (high) |
Antidepressants, SSRI (selective serotonin reuptake inhibitor): citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline (none or low) |
Antidepressants (others): bupropion, venlafaxine, mirtazapine, nefazodone, trazodone (none) |
Antiemetic and gastrointestinal: prochlorperazine (low); metoclopramide, domperidone (high) |
Antihypertensives: verapamil, methyldopa (none or low) |
Opioid analgesics: methadone, morphine, others (transient increase for several hours following dose) |
Nevertheless, the causes of slight galactorrhoea could be several and sometimes unpredictable. A synopsis of them, including also mechanical and neurogenic triggers, is listed in Table 10.3.
Table 10.3
Potential causes of slight, normoprolactinaemic galactorrhoea
Endocrine changes | Oral contraceptives |
Hypothyroidism | |
End-organ hypersensitivity to normal or low levels of prolactin | |
Medicaments’ effect | (See Table 10.2) antipsychotics, antidepressants, antiemetic and gastrointestinal, antihypertensives, opioid analgesic |
Herbal supplements | Fennel, anise or fenugreek seed, cocaine or opioid |
Mechanical causes | Excessive breast stimulation associated with sexual activity |
Frequent breast self-exams with nipple manipulation | |
Skin rash on the chest or prolonged clothing friction | |
Neurogenic stimulation | Stresses |
Chest wall surgery, trauma or burns | |
Spinal cord damage due to injury, surgery or tumours |
True galactorrhoea is always extramammary in origin and must be considered a manifestation of functional activity due to increased prolactin as a result of various causes that affect the pituitary gland. With high levels of prolactin, galactorrhoea is very clear and spontaneous, sometimes associated with amenorrhoea. Patients should undergo in-depth investigations including hormonal assay of prolactin after stimulation with TRH and, in case of abnormal levels, MRI of the sella turcica. An endocrinologist referral could be needed.
COLOURED OPALESCENT DISCHARGE. Coloured opalescent discharge may have many causes.
Fibrocystic changes secretions. In the group of coloured opalescent discharge, yellow, brown, green and grey fluids can be observed from multiple ducts. The appearance of the fluid is associated with fibrocystic changes in many patients, due to regressive, and at the same time secretive, phenomena. The initially clear and opalescent tone with time becomes more colourful with tinges that turn to beige, tan, grey or grey-green. Discharge occurs for an ectasia of the major ducts, which can be more or less marked and affect a variable number of them, initially limited and subsequently increased. Secretion is found in the same fluid component of the cyst and galactography can sometimes show a communication between cyst and dilated ducts.
Mammary duct ectasia. When duct ectasia phenomena are more marked, as observed with some fatty breasts, dystrophic secretions are mostly fluid or viscous, slightly opalescent with changeable patterns of consistency, which can range from flowing to very dense. In particular, when the dilation of main retroareolar ducts is strong and diffuse (ectatic dystrophy of retroareolar ducts), the secretion appears thicker and creamy, yellowish and ointment-like, due to an abnormal accumulation of cellular debris and lipids (Fig. 10.3).

Fig. 10.3
Toothpaste-like secretions of the breast due to dense inspissation of the secretion (comedones)
Colostrum-like or foam cells, amorphous cellular debris, lipoid debris and crystalline bodies are the ultimate expression of involution and degeneration phenomena of the epithelium of the ducts (Fig. 10.3). In this complex symptomatology of duct ectasia/periductal mastitis (see Sect. 9.2.2), episodes of galactophoritis can be observed with sporadic and momentary secretion of blood concomitant with the normal secretions.
As part of the same framework, the galactophoritis may evolve into an acute noninfective colliquation that can find a natural way out to the outside through a duct. A gentle pressure, in order to elicit the purulent discharge, sometimes allows complete drainage of the abscess-like collection (Fig. 8.6).
BLOODY AND BLOOD–RELATED DISCHARGE




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
