Fig. 31.1
Acinetobacter baumannii colonization and impaired blood flow

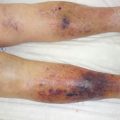
Fig. 31.2
Acinetobacter baumannii colonization and impaired blood flow
Ecthyma gangrenosum (EG) is a well-recognized but rare case of cutaneous infection most often associated with a Pseudomonas aeruginosa bacteremia. Fungal and bacterial organisms, such as Escherichia coli and Citrobacter freundii, have been identified less often as the cause of EG. EG usually occurs in immunocompromised patients and is almost always a sign of pseudomonal sepsis. The characteristic lesions of EG are hemorrhagic pustules that evolve into necrotic ulcers. This clinical entity should be considered when otolaryngologists are asked to evaluate necrotic cutaneous lesions of the head and neck [4].
Syphilis is caused by a bacterium called Treponema pallidum. Syphilis remains a major health problem, and in spite of excellent methods for diagnosing and treating syphilis, the disease is still widespread. Syphilis is called the big faker because of its numerous and atypical clinical presentations. Cases of extensive necrotic plaques have been reported in patients with an HIV coinfection [5].
31.3 Mycobacteria
Mycobacteria affecting the skin like Mycobacterium tuberculosis or marinum are more frequently associated with chronic ulcers than with extensive skin necrosis (Fig. 31.3).

Fig. 31.3
Ulceration caused by mycobacterial infection
Mycobacterium ulcerans is the causative agent of Buruli ulcer. Buruli ulcer is a chronic debilitating skin and soft tissue infection that can lead to permanent disfigurement and disability. The bacterium is most prominent in tropical regions of Africa, Asia, Australia, and South America. Infection occurs through unknown environmental exposure; human-to-human infection is rare. The frequent clinical presentation is a deep, rapidly developing chronic ulcer associated with necrosis of subcutaneous fat. Bacteriological identification is not always possible. The pathogenic effect of the mycobacterium ulcerans is due to the production of a necrotizing exotoxin with an immunosuppressive effect. Surgery is usually urgently required. The Buruli ulcer is now identified as a major public health problem in Africa [6].
Leprosy is caused by Mycobacterium leprae, an acid-fast, rod-shaped bacillus. The disease mainly affects the skin, the peripheral nerves, mucosa of the upper respiratory tract, and the eyes. It once affected every continent, and it has left behind a terrifying image in history and human memory – of mutilation, rejection, and exclusion from society. Lucio’s phenomenon is a variant of type 2 leprosy reaction, and its clinical presentation is characterized by a necrotizing erythema. It is a rare condition that occurs in patients who were never treated or in those who have followed treatment irregularly. Lucio’s phenomenon may reach severe proportions and cause death by disseminated intravascular coagulation and/or septicemia [7].
31.4 Viruses
The herpes viruses family and more specifically the herpes simplex and herpes zoster member are associated with cutaneous necrosis. Herpes simplex type 1 most commonly causes cold sores. It can also cause genital herpes. Herpes simplex type 2 is the usual cause of genital herpes, but it also can infect the mouth. Herpes zoster is the causal agent of varicella (chickenpox) and zona. The diagnosis of herpes infection has to be discussed in immunodeficient patients with extensive cutaneous necrosis [8].
Recently, cases of limited cutaneous necrosis have been described in young children who have been exposed to domestic rats. The necrosis was caused by the cowpox virus. Cowpox virus is part of the Orthopox virus genus, like variola virus, and is generally transmitted to humans by infected cats or rodents. The cowpox virus infection should be kept in mind when macular, vesicular, or necrotic cutaneous wounds do not improve with antibiotics [9].
Chronic hepatitis C infection is strongly associated with types II and III mixed cryoglobulinemia and occasionally associated with type I cryoglobulinemia.
Mixed cryoglobulinemia secondary to hepatitis C virus infection can involve the skin, and the development of a necrotizing vasculitis is observed in only 2–3 % of patients with hepatitis C virus-related mixed cryoglobulinemia. The circumstances predisposing the infected patients to develop these manifestations remain unknown [10].
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


