Chapter 21. Neck Lift
Olubimpe A. Ayeni, MD, MPH, FRCSC;
Samuel J. Lin, MD, FACS; Thomas A. Mustoe, MD
INDICATIONS
The stigmata of an aging face manifest in the neck as lipodystrophy, medial or lateral platysmal bands, and jowls. These changes can occur as a result of skin laxity, attenuation of the masseteric cutaneous ligaments, accumulation of fat below the mandibular border or under the platysma, and ptosis of the platysma. Prominent submandibular glands or digastric muscles can also contribute to the appearance of an aged neck. In some individuals, a recessed chin and a prominent, low-set hyoid can accentuate this aged appearance.
Neck rejuvenation is usually performed in conjunction with facial rejuvenation, but this procedure can be performed by itself. Nonsurgical options for neck rejuvenation include injections (injectable fillers and botulinum toxin type A), chemical peels, and laser ablation. Surgical options include facelifting, submental liposuction, plastysmaplasty, neck sling/cervical suspension, and anterior cervicoplasty. More specifically, surgery on the neck can consist of a skin lift only, reapproximation of the medial borders of the platysma muscle, transection of the platysma muscle, or division of medial platysmal bands with superolateral elevation of the muscle.
PREOPERATIVE EVALUATION
The preoperative examination of the patient begins with a global assessment of skin quality and the degree of skin laxity (Fig. 21-1). Both static and dynamic evaluation of the neck should be performed. The amount of preplatysmal submental and submandibular fat deposits should be palpated, and the presence of malpositioned or ptotic submandibular glands should be noted. According to Ellenbogen and Karlin, there are 5 criteria for a youthful neck: (a) a distinct inferior mandibular border from mentum to angle with no jowl overhang; (b) subhyoid depression; (c) visible thyroid cartilage bulge; (d) visible anterior border of the sternocleidomastoid muscle; and (e) cervicomental angle between 105 and 120 degrees, or a sternocleidomastoid to submental line with an angle of 90 degrees. The relationship between the neck and the chin must also be assessed. The nose-chin-lip plane is defined as a line extending from a point half the distance of the ideal nasal length through the upper and lower lip vermilion. The ideal chin projection is 3 mm posterior to the nose-lip-chin plane.
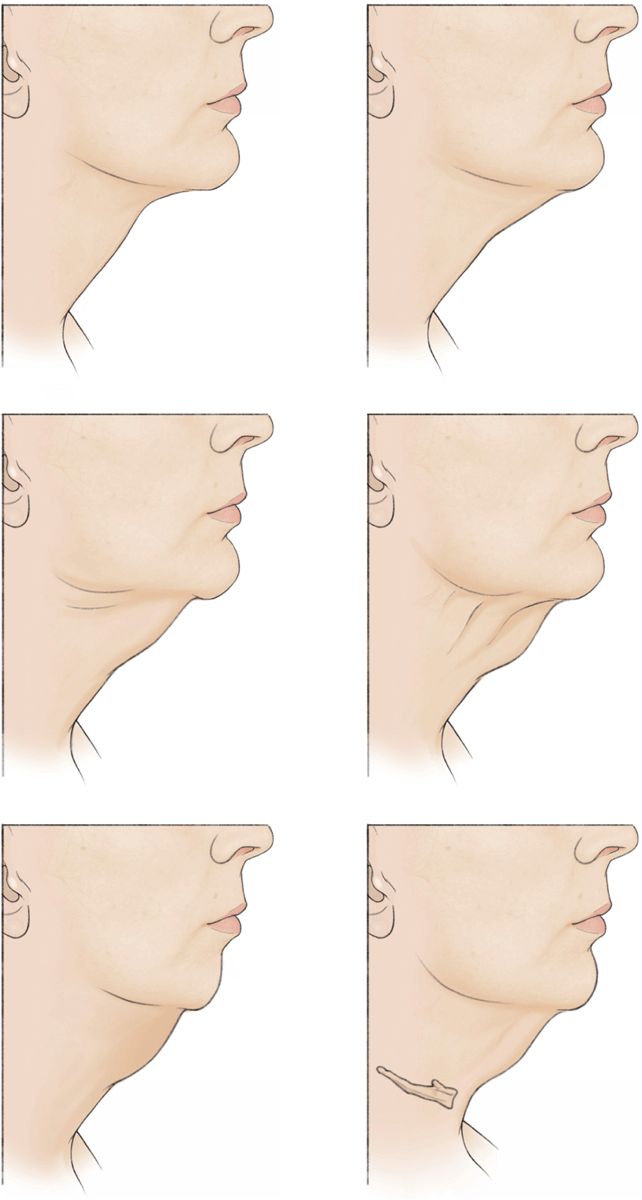
Figure 21-1 Grades of neck laxity.
Dynamic evaluation consists of watching the patient while talking. The patient is then asked to animate to accentuate potential medial or lateral platysmal banding. If the patient has jowls, the contribution of the skin, subcutaneous fat, platysma, and the submandibular gland to this deformity is recorded. Anterior, lateral, and oblique photographs should be obtained.
ANESTHESIA
Neck lifting can be performed under local anesthesia only, local anesthesia with sedation, or general anesthesia, depending on the extent of surgery to be performed. It is crucial that all preoperative markings be made before local anesthesia is infiltrated and with the patient in the upright position. The ideal cervicomental crease is identified using a paper tape measure. This line varies between patients, but is approximately at the level of the hyoid bone.
DETAILS OF PROCEDURE
A customized surgical approach is used to address the specific areas to be corrected with a neck lift. For patients who have fat deposits with excellent skin tone, lipectomy is a good option and suction or ultrasound-assisted liposuction can be performed through an incision placed behind the submental crease. If more aggressive lipectomy is required, two incisions anterior to the mastoid can be used for greater access.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


