, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
28.1 Smooth Muscle Hamartoma
28.1.1 Clinical Features
Most smooth muscle hamartomas are congenital, although acquired lesions have been described. Prevalence is greater in males [1]. Smooth muscle hamartomas present as skin-colored to hyperpigmented indurated plaques, which may have concomitant hypertrichosis and perifollicular papules or accentuation. Pseudo-Darier sign may be present and transient piloerection is seen after the lesion is rubbed. Proportional enlargement with patient growth may occur with associated hypertrichosis, pigmentation, and induration [1]. Lesions most commonly occur on the trunk and proximal extremities. Since these lesions are benign, excision is not required.
28.1.2 Histology
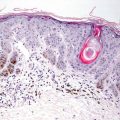
A smooth muscle hamartoma is a proliferation of haphazardly oriented smooth muscle bundles arising from the arrector pili muscles in the reticular dermis (Fig. 28.1 and Fig. 28.2) [2]. There is no cytologic atypia or mitotic activity in the lesion [3]. The lesion is poorly circumscribed. In some cases, there may be overlying hypertrichosis [4]. The relationship between a smooth muscle hamartoma and a Becker’s nevus is still uncertain, and these two entities may represent a spectrum along the same hamartomatous process [5–7].
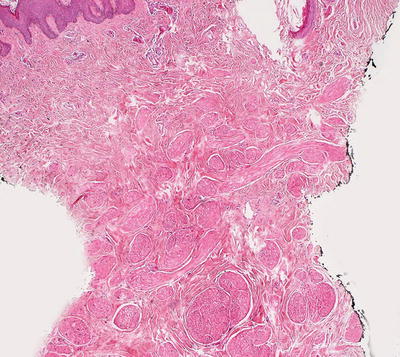
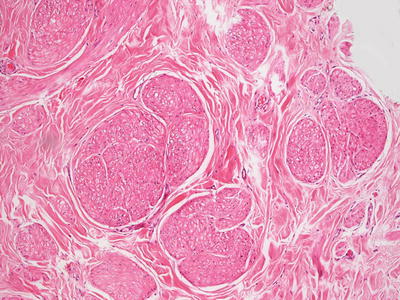
Fig. 28.1
A diffuse proliferation of mature smooth muscle bundles lacking in cytologic atypia is seen in smooth muscle hamartoma
Fig. 28.2
Abundant fascicles of smooth muscles are present throughout the dermis in smooth muscle hamartoma
The differential diagnosis includes leiomyoma. In leiomyoma, the proliferation of smooth muscle cells is better organized into bundles and appears more sharply circumscribed. Occasional mitoses may be seen.
28.2 Striated Muscle Hamartoma
28.2.1 Clinical Features
Striated muscle hamartoma is an unusual benign cutaneous lesion. Although typically congenital, it may sometimes appear in an older child or adult [9]. Lesions most commonly occur on the midline head and neck, but they have been reported in other locations, including the vagina, perianal area, tongue, and toes. Striated muscle hamartoma appears as a non-tender skin-colored nodule or tag, ranging from a few millimeters up to 2 cm in size [10]. Most lesions are solitary, but multiple lesions have been reported. Treatment consists of surgical excision .
28.2.2 Histology
Haphazard fascicles of striated muscles course throughout the dermis and the subcutis in a striated muscle hamartoma (Fig. 28.3). These muscle fibers are mature, and do not have cytologic atypia or mitotic activity (Fig. 28.4). Striated muscle hamartoma has been associated with hemangiomas [11].
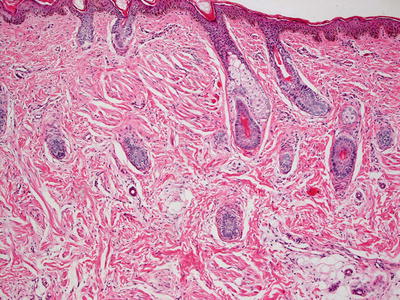
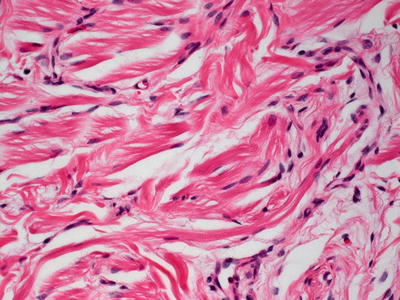
Fig. 28.3
Striated muscle bundles course haphazardly throughout the dermis in striated muscle hamartoma
Fig. 28.4
Striations are clearly visible on histologic sections in striated muscle hamartoma
28.2.3 Pathogenesis
Striated muscle hamartoma (also called rhabdomyomatous mesenchymal hamartoma ) is comprised of skeletal muscle, adipose tissue, and adnexal structures [12, 13]. The pathogenesis of striated muscle hamartoma is not known, but theories regarding genetic predisposition and abnormalities in the migration of mesodermal tissue during embryogenesis have been proposed [14, 15].
28.3 Leiomyoma
28.3.1 Clinical Features
Multiple piloleiomyomas are the most frequently reported variant of cutaneous leiomyoma. Additional subtypes include solitary piloleiomyoma and solitary genital leiomyoma [1]. Most leiomyomas occur in adults during the second and third decade of life, and there are rare reports of congenital lesions [16]. Multiple piloleiomyomas present as painful, reddish brown, indurated nodules in grouped or even dermatomal pattern [1]. Lesions most commonly occur on the extensor extremities, followed by the trunk, face, and neck. Most patients present with at least two affected body sites.
Leiomyomas have an indolent course with persistence and expansion of old lesions and development of new ones [1]. Spontaneous resolution is not likely, and lesions frequently recur following excision. Female patients with multiple leiomyomas may be at increased risk for uterine leiomyomas. Even more rarely, leiomyosarcoma may occur in affected individuals.
28.3.2 Histology
Leiomyoma is as a proliferation of smooth muscle bundles in the dermis (Fig. 28.5). The overlying epidermis is generally unremarkable or flattened, but epidermal hyperplasia can be seen in some cases [17]. Cutaneous leiomyomas arise from smooth muscle bundles within the arrector pili or from vascular smooth muscle. Tumors arising from arrector pili are more superficially located in the dermis and less well circumscribed. In leiomyomas, bundles of eosinophilic cells with ample cytoplasm and blunted, spindle-shaped nuclei course throughout the dermis (Figs. 28.6 and 28.7). Cytologic atypia is usually minimal, and mitoses are rare. The tumor cells are arranged in fascicles, and may have a whorled appearance. Leiomyomas that arise from vascular wall smooth muscle tend to occur deeper within the reticular dermis and are more sharply circumscribed. In many cases, the tumor grows concentrically around a central blood vessel that can be identified on routine tissue sections. Genital leiomyomas are more infiltrative in appearance, and smooth muscle bundles are separated by bundles of collagen. Some authors suggest that the tumor cells are more slender in appearance in this location [18].

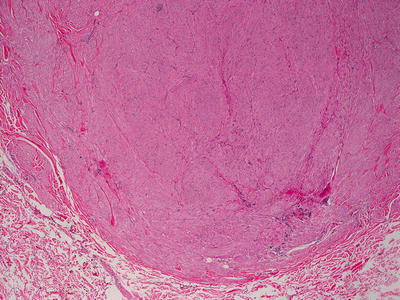
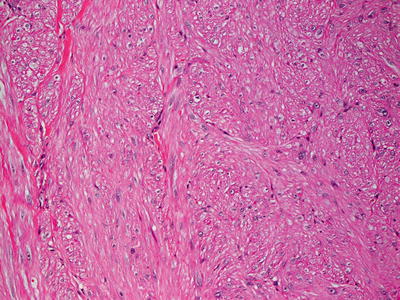
Fig. 28.5
Fascicles of smooth muscles are present in increased numbers in the dermis. They are well circumscribed in most cases, and are slightly different in color than the surrounding dermal collagen
Fig. 28.6
A well-circumscribed nodule comprised of smooth muscle fascicles is seen in leiomyoma
Fig. 28.7
Mature smooth muscle myocytes with eosinophilic cytoplasm and relatively blunted nuclei are seen in leiomyoma
28.3.3 Pathogenesis
Cutaneous leiomyoma often arises from arrector pili muscle that attaches to the hair follicle [1]. Leiomyoma can occur as solitary or multiple lesions [22]. There is no significant histologic difference between solitary and multiple leiomyomas. However, the pathogenesis of multiple leiomyomas is unique. Multiple leiomyomas can be inherited in an autosomal-dominant manner in a cancer syndrome known as Reed syndrome or hereditary leiomyomatosis and renal cell cancer (HLRCC) syndrome , in which affected individuals develop multiple cutaneous leiomyomas, uterine leiomyomas, and renal cell cancer [23]. It has been established that HLRCC syndrome is associated with mutations in the fumarate hydratase (FH) gene [24]. FH is an enzyme in the Krebs cycle responsible for the conversion of fumarate to malate. Germline FH mutations have been found in a large percentage of families with clinical features suggestive of HLRCC syndrome [25]. Mechanistically, loss-of-function mutations in FH can lead to activation of the hypoxia-inducible factor 1 (HIF-1) pathway as well as increased expression of HIF-1-regulated genes important for tumor angiogenesis, such as vascular endothelial growth factor (VEGF) [26].
28.4 Osteosarcoma
28.4.1 Clinical Features
The skin is rarely the site of primary or metastatic osteosarcoma [27]. Osteosarcoma most commonly affects children and adolescents with median age at diagnosis of 17–18 years of age [27, 28]. No gender predilection has been described. Cutaneous osteosarcomas are described as firm nodules near the site of the primary tumor, and may present as solitary lesion or multiple lesions. Cutaneous metastasis may be a hallmark of more widespread metastatic disease.
28.4.2 Histology
Osteosarcoma involving the skin is quite rare [27]. While most cases are metastatic lesions, primary cutaneous osteosarcomas have been reported [29–35]. In either situation, the tumor appears as a dermal proliferation of atypical spindle-shaped cells with marked nuclear pleomorphism, cytologic atypia, mitotic activity, and frequently multinucleated osteoblasts (Fig. 28.8). Eosinophilic osteoid material is produced by the tumor [29, 31, 36] (Fig. 28.9). A chondroblastic variant has also been reported as arising in the skin [37]. A form of carcinosarcoma is described in which there are features of basal cell carcinoma comingled with features of osteosarcoma. This neoplasm has not been seen in children [38].
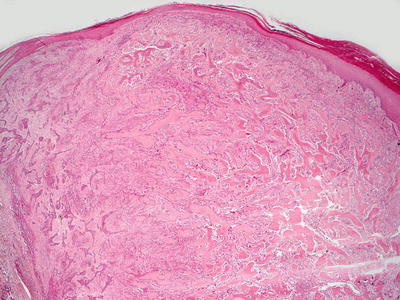
Fig. 28.8




Osteosarcoma demonstrates osteoid formation admixed with a proliferation of atypical cells in the dermis
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
