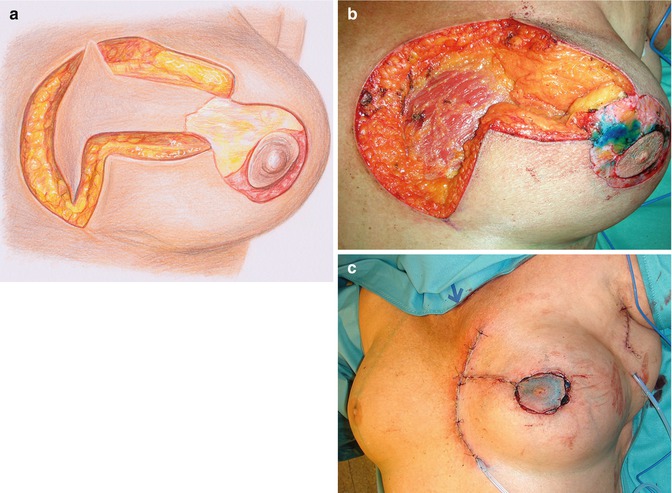
Fig. 37.1
(a–c) Preoperative view. (a) The tumor was in the upper inner quadrant (parasternal region). The scar resulted from the previous incisional biopsy. (b, c) Drawings for modified reduction mammoplasty with the joist of the T in the parasternal region
37.2 Surgery
Due to the aggressive type of the cancer, a wide quadrantectomy using a modified reduction mammoplasty with the basis of the T being in the inner quadrant was planned (Fig. 37.1b, c). Following quadrantectomy (resection weight: 420 g), the gland was dissected off the major pectoral muscle to allow adequate mobilization and closure of the defect without tension. The skin around the areola was de-epithelialized and the areola was recentralized (areolapexy) into the new center of the breast (Fig. 37.2a–c). Sentinel node biopsy was done through a separate incision in the axilla and revealed 2 negative nodes.
 Doughnut Lumpectomy: Caveat II
Doughnut Lumpectomy: Caveat II
 Doughnut Lumpectomy: Caveat I
Doughnut Lumpectomy: Caveat I
 Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
 Segment Resection of a Breast Cancer in the Submammary Fold Using a Vertical Reduction Technique
Segment Resection of a Breast Cancer in the Submammary Fold Using a Vertical Reduction Technique
 Correction of a Postlumpectomy Deformity Scar by Lipofilling
Correction of a Postlumpectomy Deformity Scar by Lipofilling
 Nipple-Areolar Complex (NAC) Reconstruction: Good Case
Nipple-Areolar Complex (NAC) Reconstruction: Good Case




Related posts:
Doughnut Lumpectomy: Caveat II
Doughnut Lumpectomy: Caveat I
Oncoplastic Superior-Based Pedicle Reduction Mammoplasty and Defect Reconstruction with an Inferior Pedicle
Segment Resection of a Breast Cancer in the Submammary Fold Using a Vertical Reduction Technique
Correction of a Postlumpectomy Deformity Scar by Lipofilling
Nipple-Areolar Complex (NAC) Reconstruction: Good Case
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
