(1)
Department of Neurosurgery Faculty of Medicine, Saga University, Saga, Japan
Keywords
Internal auditory canalFacial nerveVestibulocochlear nerveInternal auditory arterySubarcuate arteryVestibular schwannomaVestibular schwannoma surgery14.1 Introduction
For surgeries for tumors in the cerebellopontine angle (CPA), such as vestibular schwannoma, and for microvascular decompression (MVD) for hemifacial spasm (HFS) a detailed knowledge of the microsurgical anatomy of the internal auditory canal (IAC) and related neurovascular complex around the porus acusticus internus (PAI) is essential [8, 11, 20–22]. This knowledge enables detailed understanding of the preoperative images, leading to accurate preoperative prediction and intraoperative identification of the nerves, e.g., cranial nerves (CNs) VII and VIII, and blood vessels [20, 22].
The IAC was briefly mentioned in Chap. 8; in this chapter, we will describe it in more detail with a focus on arteries around the IAC. We will also explain the basic step-by-step procedure for removing vestibular schwannomas from an anatomical perspective.
14.2 The IAC and CNs VII and VIII
The IAC is approximately 10 mm long and lies in the middle part of the lateral wall of CPA—the petrous bone; PAI opens into the cerebellopontine cistern (Fig. 14.1a). The IAC is trumpet-shaped with PAI wider than the fundus of the IAC [10, 20].
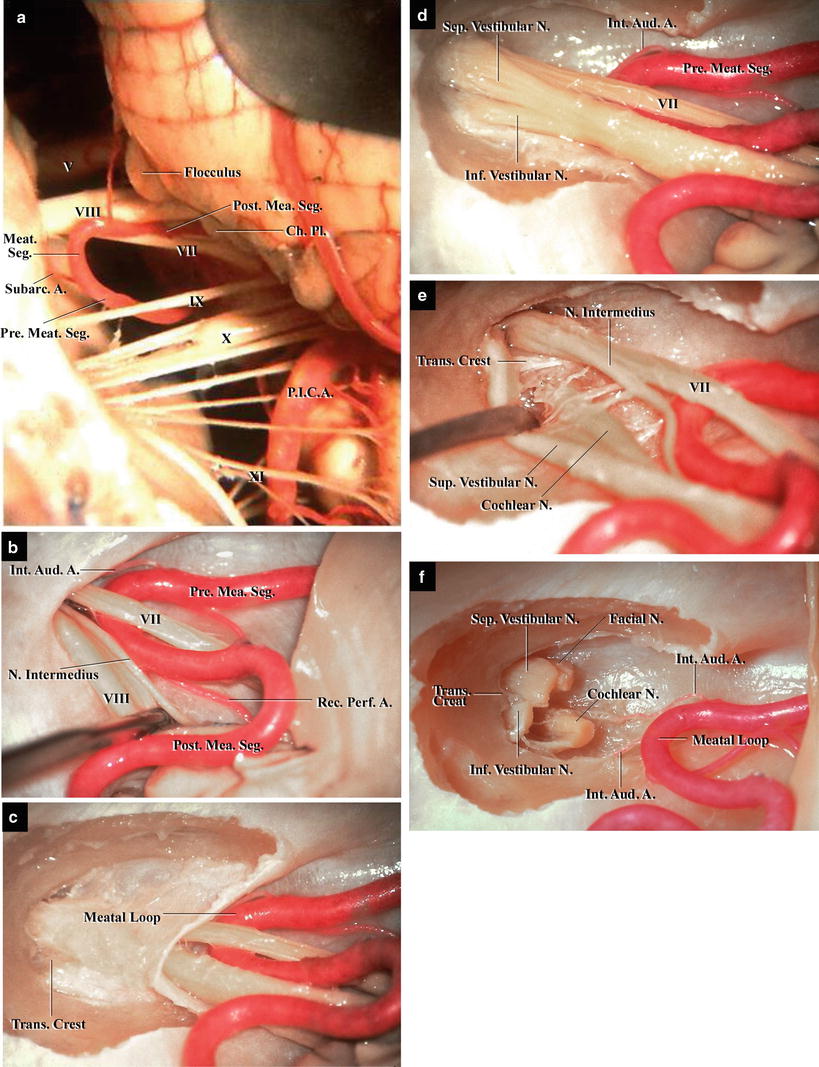
Fig. 14.1
The internal auditory canal (IAC) and cranial nerves (CNs) VII and VIII (from Matsushima T [7] with permission). (a) Left cerebellopontine angle, posteroinferior view. CNs V, VII, VIII, IX, X, and XI can be seen. The flocculus is situated superior to CNs VII and VIII. The anterior inferior cerebellar artery (AICA) forms a meatal loop immediately in front of the porus acusticus internus (PAI). (b) Left PAI, posteromedial view. CN VIII has been retracted posteriorly, revealing the nervus intermedius. AICA passes between CNs VII and VIII, forming a meatal loop. It gives rise to the internal auditory and recurrent perforating arteries. (c) Left IAC, posteromedial view. The posterior wall of the canal has been removed, exposing the dura mater. The transverse crest can be seen. (d) CNs VII and VIII are visible inside the canal after opening the dura mater. CN VIII splits into the superior and inferior vestibular nerves in the lateral portion of the canal. (e) The cochlear nerve and nervus intermedius. The vestibular nerves are retracted, revealing the cochlear nerve. The nervus intermedius courses between CNs VII and VIII. The transverse crest is also visible at the lateral end. (f) Four CNs at the lateral end of the IAC. CNs VII and VIII have been cut. They are completely separated into four nerves
CNs VII and VIII and the nervus intermedius originate from the lateral part of the pontomedullary sulcus and course into PAI. CN VIII is thicker than CN VII because it is composed of three nerves—cochlear, superior vestibular, and inferior vestibular nerves. When using the lateral suboccipital retrosigmoid approach, CNs VII and VIII are evident as two nerve bundles in the cerebellopontine cistern (Fig. 14.1a, c). In the IAC, these two bundles gradually separate 3–4 mm medial to the fundus into cochlear, superior vestibular, inferior vestibular, and facial nerves (Fig. 14.1d–f). The transverse crest separates the fundus into two parts: the upper part consisting of the superior vestibular area and facial canal and the lower part consisting of the inferior vestibular and cochlear areas (Fig. 14.1e). The vertical crest separates the superior vestibular area from the facial canal. The facial, cochlear, superior vestibular, and inferior vestibular nerves course in the respective compartments, occupying the anterosuperior, anteroinferior, posterosuperior, and posteroinferior quadrants of the IAC, respectively (Fig. 14.1e, f).
It is difficult to demarcate the component nerves of CN VIII in the cerebellopontine cistern. CNs VII and VIII and the nervus intermedius can be seen as two large nerves (Fig. 14.1b). However, CN VII is often not visible posteriorly, because it runs anterior to the wider CN VIII. Other neural structures surrounding the IAC include the flocculus, choroid plexus from the foramen of Luschka, and lower CNs (Fig. 14.1a). They lie posteroinferior to CNs VII and VIII. The choroid plexus protruding from the foramen of Luschka is often adherent to CNs IX and X [10, 21].
14.3 Vestibular Schwannomas and the Facial Nerve
The major goals of vestibular schwannoma surgery are to remove the tumor and to preserve CN VII [2, 17, 20, 22, 27, 28]. Rhoton AL Jr conducted microanatomical studies of the IAC and CNs VII and VIII with an aim to clarify the relationship between vestibular schwannomas and CN VII [20, 22, 23]. Although the studies were performed on normal cadaveric specimens, the results were of great relevance to vestibular schwannoma surgery because they demonstrated how CN VII can be displaced by vestibular schwannomas. This displacement is influenced by the invariable relationships of the four nerves (facial, cochlear, superior vestibular, and inferior vestibular) coursing in their respective compartments. Tumors frequently originate from the vestibular nerves; therefore, CN VII is usually displaced anteriorly or superoanteriorly (Fig. 14.2) [22]. The anterior inferior cerebellar artery (AICA), which forms a meatal loop near the IAC, is usually displaced around the medial margin of the tumor (Fig. 14.2a).
Fig. 14.2
Illustrations showing the relationships between cranial nerve (CN) VII, the anterior inferior cerebellar artery (AICA), and a vestibular schwannoma: posterior view of the right cerebellopontine angle (from Martin RG et al. [5] with permission). (a) The facial and cochlear nerves are displaced around the anterior margin of the tumor. Both the premeatal and postmeatal segments are in their most common locations around the lower margin of the tumor. (b) The premeatal and postmeatal segments are above the tumor, a less common pattern of displacement of AICA. (c) Both the segments are displaced anterior to the tumor
During vestibular schwannoma surgery, using a CN VII stimulator is essential. It is easy to locate the exit zone of the nerve from the inferior side of the flocculus, similar to its identification when using the infrafloccular approach during MVD for HFS [8, 11]. Rhoton AL Jr noticed that CN VII could be identified at the lateral end of the IAC because of the invariability of the aforementioned four CNs; therefore, he recommended opening the IAC during the early stages in order to locate CN VII [20, 22]. CN VII can be identified at both the brainstem side and lateral end of the IAC (Fig. 14.2a). However, this nerve can be easily torn at PAI where it often fans as a result of compression by the tumor, becoming thin and fragile. Hence, great care must be taken during dissection of CN VII from the tumor around PAI to not tear it.
(Regarding the infrafloccular approach, refer to Chap. 12: “Microvascular Decompression Surgery for Hemifacial Spasm: the Lateral Suboccipital Infrafloccular Approach.”)
14.4 Arteries Around PAI and in the IAC and Neurovascular Complex
There are five arteries around the PAI:
The meatal segment of AICA or common trunk
The internal auditory artery (IAA)
The subarcuate artery (SA)
Perforating arteries (PAs) originating from the meatal loop
Recurrent PAs returning along CNs VII and VIII to the brainstem (Figs. 14.3 and 14.4) [5, 9, 12]
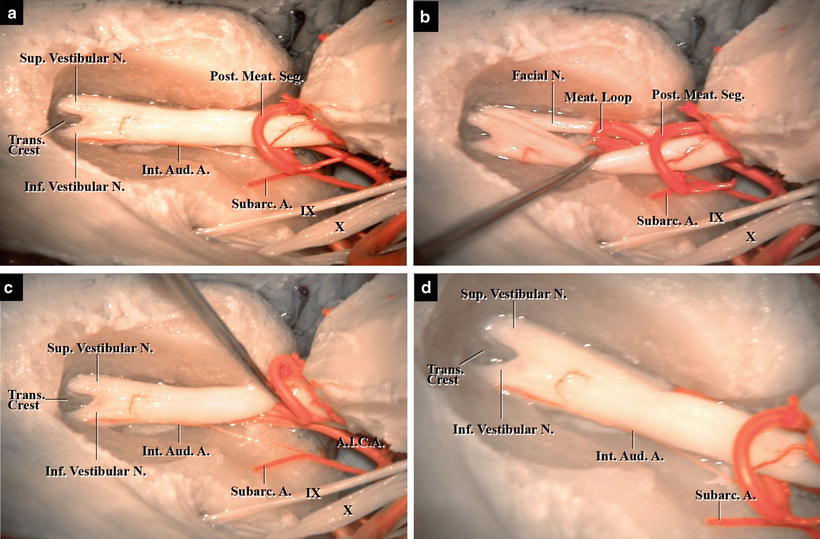
Fig. 14.3
The contents in the internal auditory canal: posterior view of a left-sided specimen with the posterior wall removed (from Matsushima T [7] with permission). (a) Opening of the dura mater. The superior and inferior vestibular nerves can be seen, separated by the transverse crest at the lateral end of the canal. (b) The meatal loop inside the canal. Cranial nerve (CN) VIII is inferoposteriorly retracted, revealing the meatal loop inside the canal. (c) The meatal segment, the internal auditory arteries (IAAs), and subarcuate artery. CNs VII and VIII are superiorly retracted, exposing the arteries. One IAA runs on the floor of the canal to its lateral end. (d) The fundus of the canal. Two IAAs are visible. One courses on the floor, and the other between the superior and inferior vestibular nerves
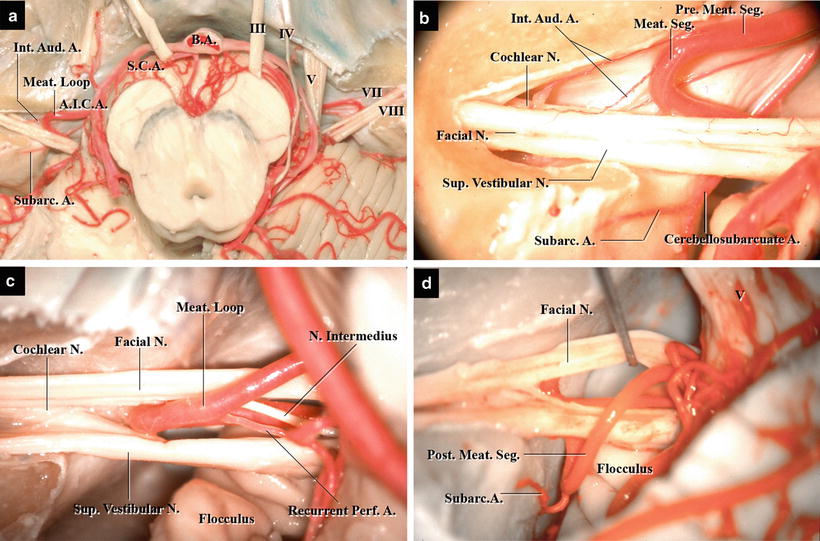
Fig. 14.4
The internal auditory canal (IAC) and surrounding arteries: superior view of the canal with its roof opened (from Matsushima T [7] with permission). (a) A specimen with the roof of the IAC opened on both sides. The anterior inferior cerebellar artery (AICA) forms a loop inside the canal on both sides. (b) The meatal loop inside the canal and the internal auditory arteries. Cranial nerve (CN) VII is located anterior to the superior vestibular nerve, and part of the cochlear nerve is visible below CN VII. AICA forms a meatal loop inside the canal. The internal auditory arteries run anterior to CNs VII and VIII, and the subarcuate artery runs below the CNs to enter the subarcuate fossa. (c) The meatal loop outside the canal and the recurrent perforating artery. CN VII is located anterior to CN VIII, while the nervus intermediate courses between CNs VII and VIII. AICA makes a meatal loop at the porus acusticus internus. The recurrent perforating artery turns toward the brainstem between CNs VII and VIII. (d) The meatal segment and subarcuate artery. CN VII has been retracted anteriorly. AICA does not form a loop. The subarcuate artery, originating from the postmeatal segment, enters the subarcuate fossa
Besides these arteries, the posterior inferior cerebellar artery (PICA) and vertebral artery sometimes reach the root exit zone (REZ) of CN VII. AICA, arising from the basilar artery, usually passes around the lower pons, turning at the supraolivary fossette to form the meatal loop in front of PAI. Subsequently, it runs to the petrosal (lateral) cerebellar surface. The meatal segment of AICA gives rise to branches, such as IAAs, immediately in front of PAI, then forms a neurovascular complex with CNs VII and VIII (Figs. 14.3 and 14.4) [5, 12].
14.4.1 CN VII and AICA
CN VII and AICA often make contact twice in the cerebellopontine cistern [9]: at REZ of CN VII, which sometimes causes HFS and at the distal portion of CN VII, at the neurovascular complex. In about 95 % of neurovascular complexes, the artery involved is either the main or rostral trunk of AICA. In contrast, the arteries that cause HFS by compressing REZ of CN VII comprise the caudal trunk of AICA or a caudal duplicated AICA [5, 12]. These facts are understandable given the natural course of AICA (refer to Chap. 10: “Anatomy for Microvascular Decompression Procedures: Relationships between Cranial Nerves and Vessels, Preoperative Images, and Anatomy for the Stitched Sling Retraction Technique.”)
14.4.2 The Meatal Segment
The meatal segment, which courses immediately in front of PAI, is formed by AICA, PICA, or the common trunk. This segment forms a neurovascular complex with CNs VII and VIII when it passes anteroinferiorly to posterosuperiorly in front of PAI (Figs. 14.3a, b and 14.4) [5]. This segment is further subdivided into premeatal and postmeatal segments (Fig. 14.4b–d). The former passes before the cranial nerve bundles, whereas the latter is after. These relationships are useful when identifying the arteries during surgery. When using the lateral suboccipital approach, the premeatal segment can be seen below CNs VII and VIII, whereas the postmeatal segment can be seen above them (Fig. 14.1a). Rhoton AL Jr noted that the relationship between the meatal segments and vestibular schwannoma was identical to the relationship between the meatal segments and the nerve of tumor origin in the normal anatomy [22].
The meatal segment changes direction near PAI to form a lateral convex loop—the meatal loop—that passes toward or through the meatus. The tips of the meatal loops reached the porus or protruded into the canal (maximum, 8 mm; mean, 3.4 mm) in about half the cases in our study (Figs. 14.3b and 14.4a, b) [12]. When AICA bifurcates proximal to CNs VII and VIII, either the rostral trunk or the rostral duplicated AICA forms the meatal loop. The meatal segment crosses the nerves anteriorly to posteriorly (Figs. 14.4b and 14.5); half the meatal segments course below the nerves, and half pass between the nerves, i.e., below CN VII and above CN VIII (Figs. 14.4c, d and 14.5). In the latter scenario, the meatal loop is sometimes hidden by the nerves and cannot be seen when using the retrosigmoid approach (Fig. 14.3a, b). Care should therefore be taken to avoid injury to the meatal loop, especially during the vestibular nerve transection procedure.
Get Clinical Tree app for offline access
Fig. 14.5
Illustrations demonstrating the courses of the internal auditory arteries (IAAs) and the meatal segment: superior view of the left internal auditory canal with its roof opened (from Matsushima T [7] with permission). (a) The meatal segment courses below cranial nerves (CNs) VII and VIII. Two IAAs originate from the premeatal segment and enter the IAC from the anterior side of the porus acusticus internus. One courses between CNs VII and VIII, and the other courses below the two nerves on the canal floor. (b
 The Veins of the Posterior Cranial Fossa: Nomenclature
The Veins of the Posterior Cranial Fossa: Nomenclature
 The Cerebellopontine Angle: Basic Structures and the “Rules of Three”
The Cerebellopontine Angle: Basic Structures and the “Rules of Three”
 Microvascular Decompression Surgery for Hemifacial Spasm: The Lateral Suboccipital Infrafloccular Approach
Microvascular Decompression Surgery for Hemifacial Spasm: The Lateral Suboccipital Infrafloccular Approach
 Microvascular Decompression for Glossopharyngeal Neuralgia: Surgical Approaches Depending on the Offending Artery
Microvascular Decompression for Glossopharyngeal Neuralgia: Surgical Approaches Depending on the Offending Artery
 Microsurgical Anatomy of and Surgical Approaches to the Jugular Foramen
Microsurgical Anatomy of and Surgical Approaches to the Jugular Foramen
 Microsurgical Anatomy of the Cerebellomedullary Fissure and Variations of the Transcerebellomedullary Fissure Approach
Microsurgical Anatomy of the Cerebellomedullary Fissure and Variations of the Transcerebellomedullary Fissure Approach




Related posts:
The Veins of the Posterior Cranial Fossa: Nomenclature
The Cerebellopontine Angle: Basic Structures and the “Rules of Three”
Microvascular Decompression Surgery for Hemifacial Spasm: The Lateral Suboccipital Infrafloccular Approach
Microvascular Decompression for Glossopharyngeal Neuralgia: Surgical Approaches Depending on the Offending Artery
Microsurgical Anatomy of and Surgical Approaches to the Jugular Foramen
Microsurgical Anatomy of the Cerebellomedullary Fissure and Variations of the Transcerebellomedullary Fissure Approach
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
