(1)
Department of Dermatology, Drexel University, Philadelphia, Pennsylvania, USA
Abstract
Staphylococcus aureus has been thought to play the major role in eczema, but other staphylococci, including Staphylococcus epidermidis, all of which are normal flora on everyone’s skin, also play major roles. S. epidermidis and other staphylococci become pathogenic when they make biofilms. These biofilms, produced when the organisms are exposed to salt and water in sweat, protect the bacterial colonies. They also make these once-sensitive organisms multidrug resistant. The two parameters, biofilm production and multidrug resistance, are very closely aligned, making these staphylococci exceedingly difficult to kill when they assume a pathogenic role. We have found biofilm production and multidrug resistance in all the species we have recovered. The pathogenic role of the staphylococcal species producing biofilms is to form an occlusion in the eccrine sweat duct. This initiates a series of events that creates itching, and the prototypical rash then ensues.
Keywords
BiofilmMultidrug resistance Staphylococcus aureus Staphylococcus epidermidis Sweat-duct occlusionThe clinical photographs that relate most directly to the microbiology chapter are flexural eczema (Fig. 2.1), facial-extensor eczema (Fig. 2.2), and nummular eczema (Fig. 2.3). These patterns of eczema were the ones we examined most frequently with cultures and biofilm studies.



Fig. 2.1
Flexural eczema. On the popliteal fossa is a red, oozing, vesicular plaque
Fig. 2.2
Facial-extensor eczema. On the extensor arm are hyperpigmented papules coalescing into plaques. Some have scales and some have crusting. This is very similar to lichen planus–like eczema
Fig. 2.3
Nummular eczema. On the leg are small and medium-sized pink, papulovesicular plaques. Some have scale
As regards microbiology, the first tightly held belief in the study of atopic dermatitis or eczema is that Staphylococcus aureus plays the major role in the disease. This was originally postulated by O’Brien [1], who thought it would assume a significant role in the pathogenesis of the disease. Twenty years later, in a series of experiments Leyden et al. [2] actually recovered the organism, though not in the amounts that would signify an infection. In truth, their numbers of organisms were in the tens of thousands, rather than in the tens of millions that are required for an infection. This was clearly stated in their work; but to this day S. aureus is considered the bacterium of greatest interest in the microbiology of eczema. This is a tightly held belief even though colonization of the plaques of eczema appears to be the major role of S. aureus.
Surprisingly, in addition to S. aureus, other staphylococci including Staphylococcus epidermidis, all of which are normal flora on everyone’s skin, play a major role in eczema (Table 2.1). This then is counter to the beliefs of the past 50 years. The S. epidermidis and other staphylococci, as normal flora, are not pathogenic until they replicate (which they can do rapidly) and create enough numbers to begin spinning out a biofilm. This process appears somewhat “teleological” for the organisms because the biofilms produced in this way now protect the newly formed clusters of bacteria. This biofilm also makes these once sensitive organisms multidrug resistant [3]. The two parameters, biofilm production and multidrug resistance, are very closely aligned, making these staphylococci most difficult to kill when they assume a pathogenic role, i.e., as a biofilm coating on an intravenous catheter. We have found biofilm production and multidrug resistance in all the species we have recovered.
Table 2.1
Species identification with the API Staph system*
S. aureus | 42 % |
S. epidermidis | 20 % |
S. hominis | 5 % |
S. xylosus | 5 % |
S. warneri | 5 % |
S. simulans | 5 % |
S. auricularis | 3 % |
S. capitis | 2 % |
S. caprae | 2 % |
S. chromogenes | 2 % |
Not identified | 8 % |
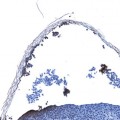
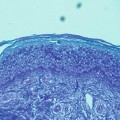
In eczema, the pathogenic role of S. aureus, S. epidermidis, or another staphylococcal species producing biofilms is to form an occlusion in the eccrine sweat duct. This initiates a series of events that creates itching, and then the prototypical rash ensues. The ductal occlusion was first noted in 1947 by Sulzberger et al. [4] (Fig. 1 in Preface); he thought it very significant, but he had no probes with which to pursue the concept. He was studying “tropical anhidrosis” for the US Army inasmuch as this condition sidelined troops for 6 weeks or more because of the heat prostration that accompanied the anhidrosis and severely lessened their readiness. The precursor to tropical anhidrosis was usually miliaria. The phenomenon was of extreme importance to the military, at that time, because one theater of the recent conflict was in the South Pacific, and many troops were affected. Of further interest Sulzberger noted ductal occlusion not only in miliaria, but in atopic eczema and in seborrheic eczema as well. A picture of an occluded duct in atopic eczema was included in the citation, but there was none from the seborrheic variant [4]. This photomicrograph convincingly displayed an occluded duct from a patient with atopic eczema. We must take on faith the diagnosis of atopic eczema, but Sulzberger was a master clinician as well as a brilliant research scientist.
These observations of Sulzberger tie eczema to miliaria, which is a disease created by occluded eccrine sweat ducts. This ductal occlusion in miliaria is not controversial, and it has been perhaps most elegantly displayed in the work of Hölzle and Kligman [5]. Other investigators, such as Dobson and Lobitz [6], have shown similar findings.
The other finding that ties miliaria to eczema is found in the work of Mowad and Leyden. They found that the only bacterium they could easily recover from the skin that would create anhidrosis and thus be important in the disease was biofilm-producing (or slime-producing) S. epidermidis [7]. Subsequently, the observation of occluded ducts in eczema, similar to the observation of occluded (with periodic acid–Schiff [PAS]-positive material) ducts in miliaria, helped form the hypothesis for the investigation that we have undertaken on several fronts. The production of anhidrosis by biofilm-producing organisms in miliaria and the decrease in sweat production in atopic eczema were important observations to include in the hypothesis as well.
Our first investigations were epidemiologic, in which we studied the various presentations in our clinic. The incidence of the disease (10.9 %) [8] that we saw changed little over 30 years [9]. We did not study the prevalence, but various studies show that the prevalence is almost double the incidence [10, 11]. Inasmuch as we are an inner city practice, the makeup of our clinic population was diverse, but eczema was nevertheless seen in all races and ethnicities. We did see the major presentations of the disease (flexural, facial-extensor, and nummular; Figs. 2.1, 2.2 and 2.3) in the typical age groupings. Facial-extensor disease was seen in the youngest patients, with flexural and nummular occurring at increasing ages. Females slightly outnumbered males, as has been reported in other studies [12
 Physiology
Physiology
 Immunology
Immunology
 Diseases in Which Eczema Is a Secondary Component (Meyerson’s Nevus and Doucas Kapetanakis Pigmented Purpuric Dermatosis)
Diseases in Which Eczema Is a Secondary Component (Meyerson’s Nevus and Doucas Kapetanakis Pigmented Purpuric Dermatosis)
 The Story of Eczema in Pictures
The Story of Eczema in Pictures
 Diseases with Occluded Sweat Ducts other than Eczema (Tinea Pedis, Axillary Granular Parakeratosis, and Seborrheic Dermatitis)
Diseases with Occluded Sweat Ducts other than Eczema (Tinea Pedis, Axillary Granular Parakeratosis, and Seborrheic Dermatitis)
 Clinical Presentations
Clinical Presentations




Related posts:
Physiology
Immunology
Diseases in Which Eczema Is a Secondary Component (Meyerson’s Nevus and Doucas Kapetanakis Pigmented Purpuric Dermatosis)
The Story of Eczema in Pictures
Diseases with Occluded Sweat Ducts other than Eczema (Tinea Pedis, Axillary Granular Parakeratosis, and Seborrheic Dermatitis)
Clinical Presentations
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
