21 Melomental folds
Summary and Key Features
• The melomental folds result from a variety of aging processes
• Melomental folds have been found to have a detrimental effect on self-perception as well as perception by others
• They are more recalcitrant to correction than other rhytides
• Melomental folds generally benefit from injection of a heavier weight filler in the deep dermal plane
• Cross-hatching or fanning technique is generally effective for effacing melomental folds
• Adjunctive techniques such as botulinum toxin injection of the depressor anguli oris muscles may prove helpful in this area
Injection strategies for melomental fold correction
While ultimately a treatment plan must be individualized for a given patient, there are some broad generalizations that may be made. The Validated Melomental Fold Scoring System allows for division of MMFs into four classes based on severity, as summarized in Table 21.1. An excellent and thorough discussion of this classification may be found in the article by Carruthers et al in the Further reading section. This scoring system will be used to more concisely discuss treatment strategies for patients based on the severity of their MMFs.
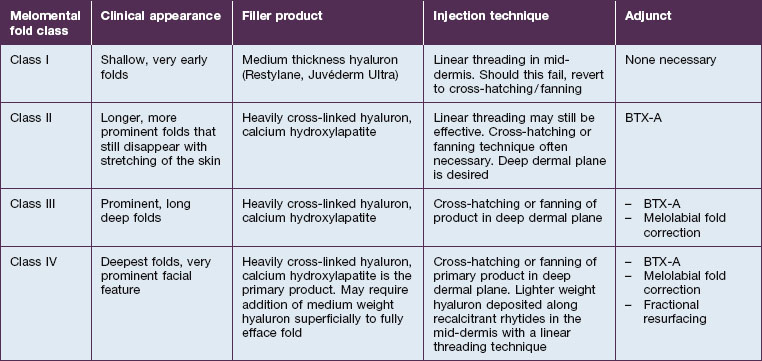
Class II folds are slightly deeper than their class I counterparts, but still will disappear upon stretching of the skin. These folds may require the use of a thicker product that consequently must be injected in the deep dermal plane. Should linear deposition of filler fail to efface these folds, a cross-hatching pattern of filler placement should be adopted. Figure 21.1 demonstrates the use of Radiesse in this area.








Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


