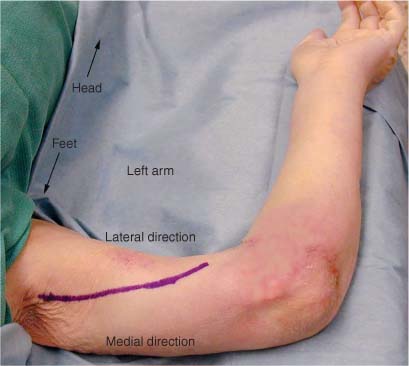
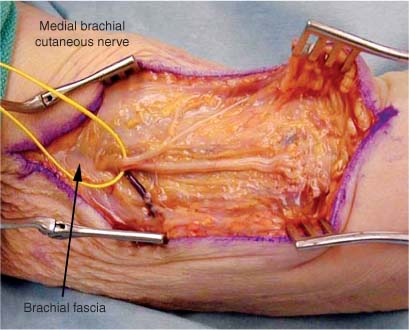
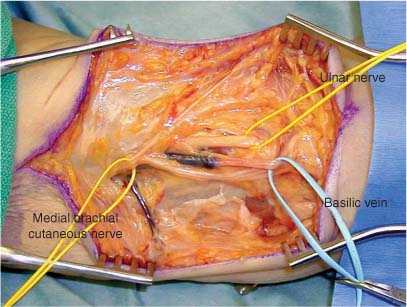
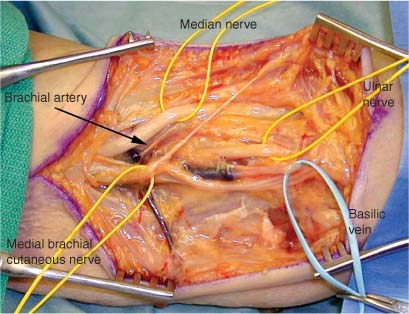
4 The median nerve arises from the medial and lateral cords of the brachial plexus. The nerve descends in the arm posterior to the pectoralis major muscle and lateral to the brachial artery. In the proximal third of the arm it lies medially in the sulcus between the coracobrachialis anteriorly and the long head of the triceps posteriorly. In the middle third it lies between the biceps brachii anteriorly and the medial intermuscular septum and the long head of the triceps posteriorly. In the distal third of the arm it lies anteromedial to the brachialis muscle and posteromedial to the biceps brachii muscle. The nerve crosses anterior to the brachial artery from lateral to medial at the midpoint of the arm. The nerve descends in the rest of the arm to the cubital fossa lying medial to the brachial artery. The median nerve innervates no muscles in the arm. The median nerve enters the cubital fossa posterior to the lacertus fibrosis (bicipital aponeurosis). This fibrous band of tissue is a tendinous insertion of the biceps brachii muscle. The nerve is medial to the brachial artery and anterior to the brachialis muscle. The nerve most commonly lies in the proximal forearm between the superficial and deep heads of the pronator teres. Many variations in its relationship to the heads of the pronator muscle have been described.1 Once past the pronator teres the nerve passes deep to the arch of the flexor digitorum superficialis. It descends in the forearm between the flexor digitorum superficialis and flexor digitorum profundus. It becomes more superficial at the wrist and lies just radial to the tendon of the palmaris longus.2 In the forearm the median nerve supplies the pronator teres, flexor carpi radialis, and flexor digitorum superficialis. The anterior interosseous nerve branches from the median nerve just proximal to the arch of the flexor digitorum superficialis and 5 to 8 cm distal to the medial epicondyle. As it passes between the flexor digitorum profundus and superficialis it goes on to innervate the pronator quadratus, the flexor digitorum profundus I and II, and the flexor pollicis longus.3 It provides two to six branches to each of these muscles.4 At 5 cm above the wrist the median nerve lies immediately palmar to the flexor digitorum superficialis tendons and dorsal to the transverse carpal ligament. After passing through the carpal tunnel a motor branch to the thenar muscles arises from the radial surface of the median nerve. Many variations of the branching of this motor nerve have been described.5 In the most commonly seen variation, a recurrent branch exits the main trunk at the distal margin of the transverse carpal ligament. Branches are given off to the flexor pollicis brevis and the abductor pollicis brevis. The nerve then passes deeply to innervate the opponens pollicis from its ulnar border. After exiting the carpal tunnel and giving off the motor branch the median nerve splits into two divisions, the radial and the ulnar. The radial division further divides into the common digital nerve to the thumb and the proper digital nerve. The digital nerves also go on to supply the lumbricales muscles of the I and II digits. The patient is placed in the supine position with the arm abducted on an arm board. The shoulder is abducted and externally rotated. The forearm is placed slightly flexed and in supination. The surgeon works from between the abducted arm and the patient’s body. The sulcus between the biceps brachii and the triceps is located, palpated, and traced proximally to the anterior axillary fold. The incision is then made along this sulcus curving laterally from a point 4 cm proximal to the medial epicondyle (Fig. 4-1). The skin is infiltrated with a vasoconstrictive agent such as lidocaine 1% with epinephrine in a 1:100,00 concentration. The skin is then incised and the interval between the biceps brachii and triceps is developed and the brachial fascia incised. The medial brachial cutaneous nerve of the arm lies just superficial to the fascia (Fig. 4-2). Care should be taken to protect this nerve because damage to it may cause neuropathic pain. There are other instances when this nerve is required for grafting procedures and it may be exposed and harvested through this incision. At this point in the arm the ulnar nerve lies posteromedial to the median nerve and may in fact be dissected out first along with the basilic vein, which is in close proximity (Fig. 4-3). Care must be taken either by direct stimulation or by thoroughly checking the anatomy that the correct nerve is exposed. Further dissection, slightly more laterally, reveals the median nerve (Fig. 4-4) as it lies first lateral and then medial to the brachial artery (Fig. 4-5). If necessary, even further lateral dissection may reveal the musculocutaneous nerve (Fig. 4-6). Because there are no branches of the median nerve in the arm, the nerve is easily mobilized and traced both proximally and distally. FIGURE 4-1 Incision for exposure of the median nerve in the left arm. The patient’s head is to the upper left and the feet are to the lower left as marked. The shoulder is abducted and externally rotated. The anatomic medial and lateral direction of the arm are indicated. The forearm is placed slightly flexed and in supination on an arm board. For the incision the neurovascular bundle is palpated and marked. To extend the incision the bundle is then traced distally along the sulcus between the biceps and triceps. FIGURE 4-2 The skin and subcutaneous tissues have been incised. The medial brachial cutaneous nerve (encircled by the yellow vessel loop) is located just deep to the brachial fascia as marked. This sensory nerve should be marked and preserved if possible. FIGURE 4-3 Deep to the medial brachial cutaneous nerve the basilic vein (encircled by blue vessel loop) is encountered. Laterally and deep to the vein is the ulnar nerve. With low level (1 μV) direct stimulation positive identification of the ulnar nerve may be confirmed by observing or recording which muscles react to the stimulus.
MEDIAN AND ANTERIOR INTEROSSEOUS NERVE
ANATOMY
In Arm
In Forearm
In Wrist
POSITIONING AND SURGICAL EXPOSURE
In Arm
Median and Anterior Interosseous Nerve
Only gold members can continue reading. Log In or Register to continue







Full access? Get Clinical Tree


