Chapter 16 Managing the Open Abdomen
1 Clinical Anatomy
Management of the open abdomen does not depend so much on recognition of the anatomy of the abdominal wall but on the maintenance of the anterior peritoneal space (Fig. 16-1). If this space is maintained, there is the potential to continue to work toward closure of the abdominal wall. If this space is lost, then the surgeon must move on to protecting the viscera from the external environment and trying to obtain skin closure over the bowel.

2 Preoperative Considerations
1 Resuscitation
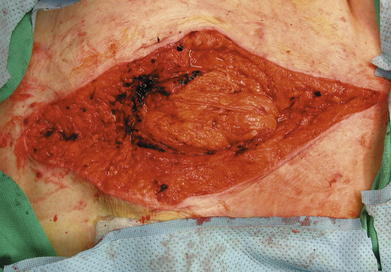
Patients who require open abdomens usually fall into one of two categories: those who still have an acute process ongoing (Fig. 16-2) and those who are in the stable phase and are in the process of having their abdomens closed (Fig. 16-3).

Those in the acute phase need to have physiologic abnormalities—acidosis, hypothermia, and coagulopathy—corrected. Providing crystalloid and blood products will accomplish this, although volume resuscitation can itself have adverse effects, specifically on intraabdominal pressure and the development of abdominal compartment syndrome (ACS). Even if the abdomen has a temporary covering in place, intraabdominal pressures need to be monitored. This is typically done with monitoring of bladder pressure. If bladder pressure is elevated or if the patient is clinically developing ACS, then the closure that was placed on the abdomen needs to be loosened to allow the viscera to expand and take pressure off of the vena cava, kidneys, and lungs.
2 Pharmacologic Management
Nutrition also can be considered a pharmacologic intervention. There is no contraindication to enteral nutrition just because the abdomen is open. Although there may be other reasons not to institute enteral feedings, the presence of an open abdomen is not one of them.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


