Chapter 17 Managing Pediatric and Neonatal Abdominal Wall Defects 
1 Clinical Anatomy
 In a patient with an omphalocele (also known as exomphalos) (Fig.17-1), the bowel and viscera, covered by a membrane composed of visceral peritoneum, Wharton jelly, and amnion, herniate through a central defect (≥4 cm) at the umbilical ring. The viscera extend into the base of the umbilical cord and the umbilical cord inserts into the apex of the omphalocele sac. The sac may contain loops of small bowel, large intestine, stomach, and liver (in 50% of cases). These viscera are otherwise functionally normal.
In a patient with an omphalocele (also known as exomphalos) (Fig.17-1), the bowel and viscera, covered by a membrane composed of visceral peritoneum, Wharton jelly, and amnion, herniate through a central defect (≥4 cm) at the umbilical ring. The viscera extend into the base of the umbilical cord and the umbilical cord inserts into the apex of the omphalocele sac. The sac may contain loops of small bowel, large intestine, stomach, and liver (in 50% of cases). These viscera are otherwise functionally normal.
 In patients with gastroschisis (Fig.17-2), the small bowel freely protrudes, without an overlying sac, through a smaller defect (<4 cm) at the junction between the umbilicus and the skin. The defect is almost always to the right of the umbilicus. The herniated contents may include small bowel, stomach, bladder, fallopian tubes, ovaries, and testes.
In patients with gastroschisis (Fig.17-2), the small bowel freely protrudes, without an overlying sac, through a smaller defect (<4 cm) at the junction between the umbilicus and the skin. The defect is almost always to the right of the umbilicus. The herniated contents may include small bowel, stomach, bladder, fallopian tubes, ovaries, and testes.



 In gastroschisis, due to exposure to amniotic fluid and compromised blood supply, the small bowel may become thick, shortened, edematous, discolored, and covered with fibrinous exudates (also known as a “peel”). This may reduce the malleability of the bowel and make manual reduction more difficult. Furthermore, extensive peel is thought to lead to a prolonged ileus after bowel reduction.
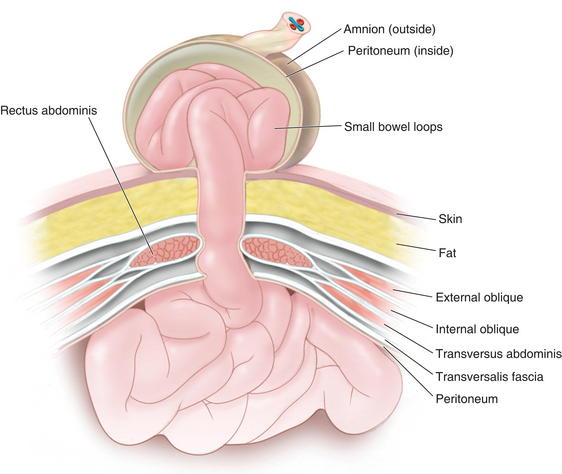
In gastroschisis, due to exposure to amniotic fluid and compromised blood supply, the small bowel may become thick, shortened, edematous, discolored, and covered with fibrinous exudates (also known as a “peel”). This may reduce the malleability of the bowel and make manual reduction more difficult. Furthermore, extensive peel is thought to lead to a prolonged ileus after bowel reduction. Omphalocele is due to the primary failure of the developing intestines to return to the abdominal cavity after migration into the umbilical cord during weeks 6 to 12 of gestation. Figure 17-3 depicts a cross-sectional diagram of the anatomy seen in omphalocele. The abdominal muscles are otherwise normally developed.
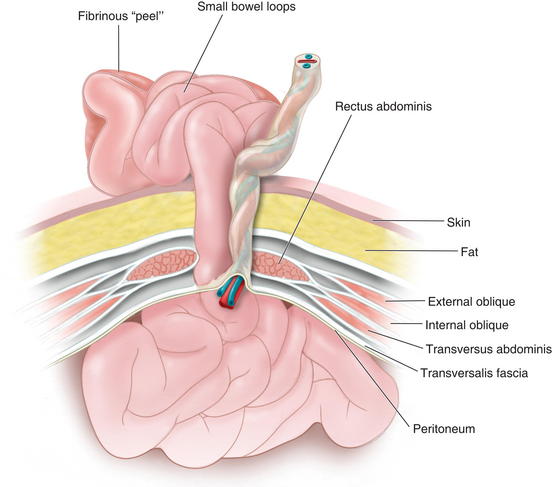
Omphalocele is due to the primary failure of the developing intestines to return to the abdominal cavity after migration into the umbilical cord during weeks 6 to 12 of gestation. Figure 17-3 depicts a cross-sectional diagram of the anatomy seen in omphalocele. The abdominal muscles are otherwise normally developed. Gastroschisis is believed to be caused by involution of the right umbilical vein during the fourth week of development. The resulting ischemia leads to a full-thickness defect in the musculature of the abdominal wall. Figure 17-4 shows a cross-sectional diagram of the anatomy seen in gastroschisis.
Gastroschisis is believed to be caused by involution of the right umbilical vein during the fourth week of development. The resulting ischemia leads to a full-thickness defect in the musculature of the abdominal wall. Figure 17-4 shows a cross-sectional diagram of the anatomy seen in gastroschisis.

2 Preoperative Considerations
 Both omphalocele and gastroschisis may be suspected prenatally with an elevated maternal serum α-fetoprotein (although this level can be normal or elevated because of other conditions) and can be diagnosed readily by prenatal ultrasonography in 75% to 80% of cases (after 14 weeks’ gestation when the fetal midgut returns to the abdomen). They can be differentiated sonographically by the presence of a sac, location of the defect, and presence of additional abnormalities. These methods have increasingly led to detection before birth and allow for prenatal education and family counseling.
Both omphalocele and gastroschisis may be suspected prenatally with an elevated maternal serum α-fetoprotein (although this level can be normal or elevated because of other conditions) and can be diagnosed readily by prenatal ultrasonography in 75% to 80% of cases (after 14 weeks’ gestation when the fetal midgut returns to the abdomen). They can be differentiated sonographically by the presence of a sac, location of the defect, and presence of additional abnormalities. These methods have increasingly led to detection before birth and allow for prenatal education and family counseling.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


