Chapter 9 Management of Gynecomastia
Gynecomastia may be defined as enlargement of the male breast. However, from a surgical point of view, it may be more helpful to view the condition as a persistent enlargement of the breast as transient breast enlargement during puberty is actually a normal finding occurring in up to 65% of normally developing adolescent boys. It is this persistence that generally motivates patients to seek treatment as the enlarged breast can create a significant contour deformity when compared to the appearance of a normal male chest contour. From a therapy standpoint, there are three main presentations of gynecomastia that require slightly different approaches when it comes to designing an appropriate course of treatment.
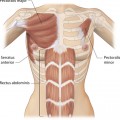
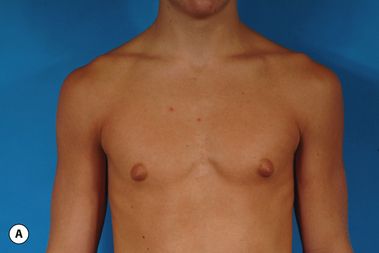
The hallmark finding in patients with adolescent gynecomastia is a firm, fibrous mass of tissue that develops directly under the areola (Figure 9.1). This mass can be variable in size and can herniate through the elastic areolar skin, resulting in a very obvious contour abnormality. In addition, it is not uncommon for a surrounding fibrofatty stroma of varying volume to develop in concert with the subareolar mass. The magnitude of this fatty overgrowth is directly related to the body habitus of the patient with more obese patients tending to demonstrate a more dramatic increase in the size of the breast (Figure 9.2). Along with the general breast overgrowth can be noted an excess of skin to the point that actual ptosis of the breast mound can be noted (Figure 9.3). Finally, as a result of the enlarged subareolar breast bud along with the general increase in the volume of the breast, the diameter of the areola can increase significantly, all of which combines to create a decidedly abnormal breast contour for a young adolescent male (Figure 9.4).





Senescent gynecomastia – Alternatively, persistent gynecomastia can develop later in life, generally after the age of 50. Here the nature of the enlarged breast is slightly different as the fibrofatty component of the breast tends to be more predominant (Figure 9.5). Generally, the patient will experience a gradual enlargement of the breast that develops over the course of a year or more and this enlargement will often be tied to an overall gain in weight. A subareolar thickening may be noted but the enlargement of the breast is more diffuse in the older male and often there will be associated fatty deposition under the arm and higher up onto the chest wall toward the clavicle. Again, a change in the ratio of the sex hormones may be responsible for this change in body habitus with the natural decline in circulating levels of testosterone that is noted with advancing age being the likely etiologic factor. These patients generally seek treatment in an effort to restore a more normal overall male chest wall contour.


One specific variant of pathologic gynecomastia is that which occurs as a result of exogenous hormone administration. Gynecomastia has been noted to develop as a result of recreational drug use with marijuana being widely recognized as a common cause of the condition. Also, young males involved in the sport of bodybuilding will sometimes develop a very discrete and fibrous subareolar type of gynecomastia secondary to the use of either injectable or oral testosterone or testosterone precursor-like drugs, along with a whole host of other anabolic steroid type substances. Screening for any history of drug use becomes particularly important in these types of patients in order to clarify the etiology of the condition and, as well, to develop an appropriately targeted treatment plan. Specifically, it is highly advisable that such patients discontinue all exogenous drug use prior to undergoing any form of surgical treatment.
Indications for Treatment
Although pain may occasionally be noted in patients with gynecomastia, it is most certainly the altered chest contour along with the emotional sequelae of the condition that motivates nearly all patients to seek treatment. This is particularly true in adolescent males. It must be recognized that the teenage years are a vitally important time period during which significant social and emotional growth occurs. In these patients, even modest cases of gynecomastia can result in social withdrawal and avoidance of any situation that will require the patient to take his shirt off. As a result, important social activities including participation on athletic teams, swimming and even casual interaction with other peers are avoided secondary to the embarrassment the patient feels about his appearance. Once gynecomastia is recognized, it is reasonable to delay definitive surgical excision for up to 2 years or more, as some patients will spontaneously regress on their own as their internal hormonal environment stabilizes. Typically, this will occur by the age of 15. However, should any degree of social withdrawal become noticeable as a result of the condition, it is entirely reasonable and recommended to proceed with surgical treatment.
Special mention must be made concerning those patients who present with gynecomastia in association with significant obesity. Certainly, in these patients, the major cause of the enlarged breast contour is the excess general fatty accumulation. Although some stromal overgrowth in the subareolar region may be present, it is generally overwhelmed by the significant amount of fat present in the breast. This combination can often lead to surprising levels of breast development that can result in significant breast ptosis (Figure 9.6). Therefore, while any first line therapy would best be directed primarily at weight loss, the adverse effect such breast development can have on a patient who is likely already struggling with body image issues can be quite damaging. For this reason, it is very reasonable and even advisable to proceed with surgical correction of gynecomastia in the obese. Normalizing the contour of the chest wall may well allow the patient to make appropriate lifestyle changes later in life as he matures that will lead to a healthier body composition.