, Madan Ethunandan2 and Tian Ee Seah3
(1)
Poole Hospital NHS Foundation Trust, Poole, Dorset, UK
(2)
Department of Oral and Maxillofacial Surgery, University Hospital Southampton NHS Trust Southampton General Hospital, Southampton, UK
(3)
Orange Aesthetics and Oral Maxillofacial Surgery, Singapore, Singapore
The cutaneous sensory nerve supply of the head and neck region is principally by the branches of the trigeminal nerve and cervical plexus, with smaller contributions from the other cranial nerves (Fig. 1.1).
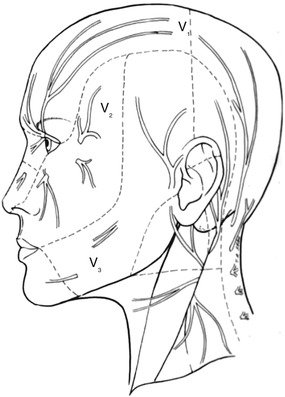
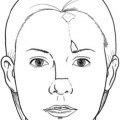
Fig. 1.1
Sensory nerve supply of the head and neck
Most of these nerves can be anaesthetised by nerve blocks, enabling surgical procedures to be carried out under local anaesthesia in addition to helping with postoperative analgesia.
Anaesthesia for Specific Areas
Forehead
Landmarks
Supraorbital Nerve: Emerges from the supraorbital foramen along the vertical plane of the pupil
Supratrochlear Nerve: Medial end of eyebrow, about 1.5 cm from midline
Technique
Supraorbital Nerve: Prepare the skin using sterile technique. Request patient to look straightahead, palpate the supraorbital ridge and locate the supraorbital notch/foramen along the vertical plane of the pupil. Insert needle and raise a small skin wheal, advance needle 3–4 mm and deposit solution superior to the foramen in a supra-periosteal location.
Supra trochlear Nerve: Insert needle at the medial end of the eyebrow, 1.5 cm from the midline and infiltrate anaesthetic in the subcutaneous tissues. Advance needle across the midline and deposit solution in a similar location to anaesthetise the contralateral nerve.
Area of Anaesthesia
Forehead up to the lateral canthus, anterior scalp up to the coronal plane
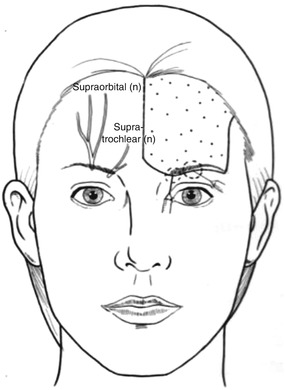
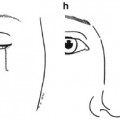
Fig. 1.2
Supraorbital, Supratrochlear nerve block
Temple
Landmarks
Zygomatico temporal Nerve: Emerges from the zygomatioctemporal foramen and pierces the temporal fascia 2.5 cm above the medial end of the zygomatic arch
Technique
Prepare the skin using sterile technique. Insert needle 2.5 cm above the medial end of the zygomatic arch, lateral to the lateral orbital rim, and deposit solution into the subcutaneous tissues.
Area of Anaesthesia
Lateral forehead, medial temple

Fig. 1.3
Zygomaticotemporal, Zygomaticofacial nerve block
Landmarks
Auriculotemporal Nerve: Arises from the mandibular division of the trigeminal nerve, passes posterior to the neck of the condyle and runs superiorly crossing the root of zygomatic arch
Technique
Prepare the skin using sterile technique. Insert needle 2 cm above the tragus, just anterior to the superior attachment of the helix to the scalp, and deposit solution into the subcutaneous tissues.
Area of Anaesthesia
Lateral temple, tragus, superior helix
Caution: Avoid intravascular injection into superficial temporal vessels
Risk of bruising, haematoma
Paralysis – temporal branch of facial nerve
Cheek
Nerves
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


