Subtypes
Most common sites of involvement
Cutaneous lichen planus
Actinic
Sun-exposed areas
Annular
Male genitalia, intertriginous
Atrophic
Predominately on lower extremities, may occur on other areas of the body
Erosive
Soles of the feet
Guttate
Trunk
Hypertrophic
Anterior legs, ankles, interphalangeal joints
Linear
Lower extremities
Follicular
Trunk and proximal extremities
Papular
Flexural surfaces
Bullous
Feet
Pigmentosus
Sun-exposed areas
Pigmentosus-inversus
Intertriginous and flexural areas
Nail
Fingernails > toenails
Palmoplantar
(1) Malleoli
(2) Soles
Lichen Planopilaris
(1) Classic- vertex scalp
(2) Frontal fibrosing alopecia
(3) Graham-Little-Piccardi-Lasseur Syndrome
Mucosal lichen planus
Oral
Reticular
(1) Buccal mucosa and mucobuccal folds
Atrophic
Attached gingiva
Hypertrophic
Buccal mucosa
Erosive
(1) Lateral and ventral tongue
(2) Buccal mucosa
Bullous
Posterior and inferior areas of the buccal mucosa
Plaque-like
Dorsum of tongue and buccal mucosa
Vulvovaginal
Vaginal introitus, clitoral hood, labia minora, labia majora, vagina
Esophageal
(1) Proximal esophagus
(2) Proximal and distal esophagus
(3) Distal esophagus (80 % have mucosal involvement)
Special forms
Drug-induced
Sun-exposed areas
Lichen planus-lupus erythematosus overlap
Distal extremities, sun-exposed
Lichen planus pemphigoides
Extremities
Cutaneous Disease
LP is characterized by four to six descriptive, repetitive “P” terms (pruritic, purple, polygonal, planar, papules and plaques). The individual lesions vary in size from a few millimeters to large, coalescent plaques (Fig. 31.1). The violaceous color of longstanding LP plaques results from the combination of red blood in the capillaries, interface lymphocytes, and the bluish-gray hue of dermal melanin [17]. Fine white lines, which represent areas of focal epidermal thickening, are termed Wickham’s Striae (Fig. 31.2). The lesions are more clearly visualized using contact dermoscopy. LP is often localized to the flexor aspects of the extremities as well as the oral and genital mucosa. The face and interfollicular scalp are typically spared. Isomorphic phenomenon (Koebnerization) (Fig. 31.3) and Wolf’s isotopic response are both seen in LP. The former represents disease at the site of prior trauma and the later represents secondary disease occurring in previously diseased skin, most commonly varicella zoster virus (VZV) [18–20].


Fig. 31.1
Classic cutaneous lichen planus (a) Left-Violaceous papules and plaques on the dorsal foot (b) Right-Violaceous papules and plaques with overlying reticulate, white striae (Wickham’s striae)
Fig. 31.2
Wickham striae: Violaceous plaque with overlying lace-like, reticulated white striae
Fig. 31.3
Koebnerization (a) Left-Linear cluster of lichenoid papules corresponding to the site of prior trauma (b) Right-Clustered papules at site of prior surgery
Nail Disease
Nail disease occurs in up to 10 % of patients with LP and the fingernails are more commonly affected than the toenails [21, 22]. LP can affect the nail folds, bed, and matrix. The most common findings are: thinning, ridging (trachyonychia), and distal splitting of the nail plate (onychoschizia) (Fig. 31.4) [22]. One study found that nail matrix involvement was associated with trachyonychia (40 %), pitting (34 %), and dorsal pteryigium (21 %) [23]. Nail bed involvement was associated with chromonychia (56 %) and nail fragmentation (51 %). Paronychia was seen in 32 % of cases and disease of all three-nail components was associated with longitudinal streaks (82 %). Similar nail patterns may be seen in alopecia areata, psoriasis, eczema, and pemphigus vulgaris.

Fig. 31.4
Nail lichen planus (a) Left– Purple, red plaques surrounding the proximal and lateral nail folds (paronychia) (b) Middle– Longitudinal ridging with forward growth of the eponychium and adherence to the proximal nail plate (dorsal pterygium) (c) Right– Longitudinal ridging of all nails (trachyonychia) with distal splitting (onychoschizia)
Mucosal Disease
LP commonly involves the oral mucosa but the penis, vulva, vagina, anus, nose, larynx, esophagus and conjunctiva can also be affected. OLP is more common in women than men (2:1). Oral involvement occurs in approximately 60–70 % of individuals with LP and may be the only site of involvement in 20–30 % [11, 24–27].
Multiple subtypes of OLP have been described: reticular, erosive, atrophic, papular, plaque, and bullous. Ulcerative OLP is the most common subtype reported in studies, likely due to symptomatology and severity of disease [26, 28]. However, clinical experience indicates that the reticular subtype is more common but patients are less likely to seek medical care due to its indolent and often asymptomatic nature. The lesions are often symmetrical and the buccal mucosa is the most common site of involvement (80–90 %) (Fig. 31.5) [25, 29–32]. Gingival involvement is uncommon, being the sole presentation in 8 % of cases, but remains the most common cause of desquamative gingivitis (75 % of cases) [33]. The classic lacy streaks (Wickham striae) are most commonly seen on the buccal mucosa. Koebnerogenic factors: smoking, dental caries and amalgams may exacerbate disease.
Fig. 31.5
Oral lichen Planus: Typical lace-like whitish, reticulated pattern (Wickham striae) on the buccal mucosa
Oral lichenoid contact stomatitis can be clinically and histologically indistinguishable from OLP. In patients with OLP, one study identified a contact hypersensitivity in 40 % of the cases [34]. The most common culprits are amalgams in fillings as well as food flavorings (cinnamon, cinnamaldehyde, and spearmint) [34–36]. Some individuals may benefit in removal of damaged and corroded fillings despite negative patch testing [37]. This may be due to false negative patch testing, which would have been picked up with other methods (repeat open application testing (ROAT)) or due to the removal of a mucosal irritant.
Genital lesions (Fig. 31.6), including vulvar, vaginal, and penile, have been reported in 19–57 % of individuals with OLP and 15–50 % of cutaneous LP [25, 38–40]. Of patients with vaginal involvement, 44–100 % have oral disease. Therefore, when examining a patient with vulvar or vaginal inflammation, an oral and cutaneous examination is essential. Vulvo-vaginal gingival (VVG) syndrome is a specific subtype of vulvar and vaginal LP with oral involvement. Genital lesions, specifically penile, often have an annular appearance.
Fig. 31.6
Genital lichen planus: Shiny white, reticulated plaque with a violet hue and a small superficial erosion on the corona
Hair Disease
Hair disease has been reported in up to 40 % of LP [43–45]. Follicular involvement on the body often occurs; however, the classic cicatrical scalp alopecias of LP are the focus. Three clinical subtypes are: classic lichen-planopilaris (LPP), frontal fibrosing alopecia(FFA), and Gram-Little-Piccardi-Lasseur Syndrome(GLPLS) [44, 46]. LP of the scalp occurs more frequently in women (5 to 31:1) with FFA dominating the most [44]. Classic LPP affects the vertex scalp and consists of diffuse erythema with perifollicular hyperkeratosis and livid erythema (Fig. 31.7) [44]. Dermoscopy can aid in the diagnosis of early scarring LPP. Dermoscopic features of LPP include: absence of follicular opening, cicatricial white patches, peripilar casts and perifollicular scale, blue-gray dots, perifollicular erythema, and polytrichia (2–3 hairs) [47]. Late stage disease and progressive disease often lead to nondescript scarring (Pseudopelade of Brocq).

Fig. 31.7
Lichen planopilaris (a) Left– Early disease with widening of the hair line and erythema of the scalp (b) Right– Dermoscopy (10× magnification) provides much higher resolution and shows classic features of lichen planopilaris: loss of follicular ostia, perifollicular scale and erythema
FFA most commonly affects postmenopausal women and is characterized clinically by a band-like alopecia of the frontal hairline [48]. Up to 75 % of women with FFA report concomitant loss of the eyebrows, which tends to be non-inflammatory [49]. Thyroid dysfunction is more common in individuals with FFA versus LPP (31 % versus 10 %) [44]. The difference seen may be partially age related. However, a more recent study found an elevated rate of thyroid dysfunction in individuals with LPP versus controls (34 % versus 11 %) [50]. The role of thyroid hormone receptors on keratinocytes, follicular function, and hair organ homeostasis remains unknown. GLPLS is a rare subtype characterized by Cicatricial alopecia of the scalp, non-scarring alopecia of the axilla and groin, and follicular papules on the trunk and extremities [51].
Special Forms
Drug-Induced Lichen Planus
Lichenoid drug eruptions (LDE) can be virtually indistinguishable from LP. LDE have been described with: oral ingestion or subcutaneous injection (angiogtensin converting enzyme inhibitors (ACEi), antimalarials, calcium channel blockers (CCB), gold, non-steroidal anti-inflammatory drugs (NSAIDs), tumor necrosis factor-alpha (TNF-α) inhibitors and contact factors (mercury, copper, gold, phenylenediamine (PPD) derivatives) [52]. Classically, LDE involve a photodistributed area, lack prominent epidermal changes, and lack mucosal involvement (with oral ingestion). LDE are typically delayed a few months from initial exposure but onset can vary from days to years [52]. LDE typically clear within a few weeks to few months after drug discontinuation. However, reactions post-gold exposure can persist for years.
Overlap Syndromes
LP pemphigoides has distinct features of both LP and bullous pemphigoid (BP) and occurs secondary to BP antigen 2 (BPAG-2) antibodies to the Medical College of Wisconsin-4 (MCW-4) epitope on the non-collagenous 16A (NC16A) domain [53]. The bullous and lichenoid lesions tend to occur on the extremities [54]. LP/Lupus erythematosus (LE) overlap has clinical, histological, and immunofluorescent features which overlap between these two entities and can have a positive anti-nuclear antibody (ANA). The extremities are commonly involved and the clinical features are atypical for LP with atrophic plaques and minimal epidermal disruption [55].
Associations with Systemic Diseases and Infections
Systemic Diseases
Patients with LP are at a higher risk of metabolic syndrome and tend to have more cardiac risk factors than healthy individuals [56, 57]. Thyroid dysfunction is found in up to 34 % of patients with LPP [50]. Lichen sclerosus et atrophicus (LS et A) is seen in up to 16 % of patients with OLP [38, 58]. OLP is associated with chronic liver disease.
Psychological and Neurogenic Factors
Increased stress, anxiety, sleep disturbance, and depression are reported in LP [59–61]. Up to 60 % of patients had chronic nervous distress or a stressful event near the time of a flare [11]. Recent studies examined the role of neural pathways and neurogenic factors in LP and showed co-localization of mast cells and nerve fibers as well as increased peripheral nerve innervation in OLP [62, 63]. The pattern of innervation appears to be different between lichenoid reactions and OLP [64]. The differences in nociceptive features are partially explained by the nature of the lesions (reticular versus erosive) rather than the innervation. Neuro-modulating drugs have been reportedly successful in OLP although larger studies verifying these findings are needed [65].
Infections
Patients with OLP and liver disease have significantly higher rates of hepatitis C (Hep C) in selected populations (78 % versus 3 %) [66]. There may be specific unidentified genetic factors contributing to this co-occurrence, as large studies on Hep C have not found LP to be a common finding [67]. Hep C and LP are associated in certain endemic regions (East and Southeast Asia, South America, the Middle East, and Southern Europe) but not in others (North America, South Asia, and Africa) [68]. In general, patients with LP have a six-fold risk of having Hep C relative to the control population [32]. The heterogeneity of Hep C and OLP may be related to the human leukocyte antigen-DR6 (HLA-DR6) haplotype, which is found in endemic regions with Hep C and LP [69, 70]. There is no strong link between hepatitis B (Hep B) and LP [71].
Other infections have been implicated in LP. Human papilloma virus (HPV) is more common in OLP with overall odds ratio (OR) of 5.12 and HPV-16 of 5.61 [72]. In addition, the higher rates of oncogenic subtypes may explain part of the increased malignancy risk. Individuals with OLP are more likely to be colonized with Candida species than controls [73]. Non-Candida albicans species were isolated in patients with OLP, particularly those with OLP and diabetes mellitus (DM) [73]. In zosteriform LP, the lesions have expressed VZV antigens. In addition to being a potential trigger of LP, VZV antigen expression may differentiate zosteriform LP from linear presentations of LP [74].
Malignant Transformation
The malignant potential of LP is dependent upon the site of involvement, clinical subtype, duration of disease, and patient population. The reported rates of squamous cell carcinoma (SCC) development have varied: 0.8 % of OLP in the United States, 1.9 % in the United Kingdom, 0.6 % in China, and 1 % in the Swedish population [75–78]. Longstanding erosive and atrophic disease appears to have the highest risk of malignant transformation. The tongue is the most common site of involvement. Other risk factors for oral SCC, including tobacco and alcohol, have not been observed at greater frequency in OLP. Candida as well as HPV have been observed in higher frequency in OLP and may be contributory [72, 73].
No overall increased risk of malignancy has been observed in cutaneous LP [78]. There are rare case reports of cutaneous SCC arising in LP. Risk factors include: hypertrophic or verrucous LP, location on the lower extremity, a history of arsenic or x-ray exposure, and longstanding disease (average of 12 years) [78].
Laboratory Tests
No specific laboratory test abnormalities are seen in LP. Hep C testing should be considered in those with risk factors as well as those in endemic areas having a prevalence of greater than 7 % [79]. Testing for dyslipemia and thyroid dysfunction (thyroid stimulating hormone (TSH) and thyroid peroxidase (TPO) antibody) is part of routine health maintenance and determining the psychosocial impact of disease is essential [50, 56, 57, 60, 61]. Individuals with a normal TSH and TPO antibodies will require follow up monitoring for the development of clinical hypothyroidism. In oral disease, allergic contact dermatitis (ACD) should be ruled out, as oral contact stomatitis can appear identical to LP [34–36, 80].
In most cases, LP is a clinical diagnosis and should be confirmed with a biopsy when atypical or overlap features are present. Dermoscopic driven biopsies showing the key features led to definitive diagnosis in 95 % of LPP cases [81]. In cases of vesiculobullous disease or erosive disease, direct immunofluorescence (DIF), indirect immunofluorescence (IIF), as well as enzyme linked immunosorbent assay (ELISA), may be needed to differentiate from other immunobullous diseases.
Pathology
Pinkus described the initial, modern understanding of the LTR which focused on the spectrum of epidermal damage to the basement membrane and its resulting cascade of events [82]. Two major pathologic findings were described, the lymphocytic LTR and consequent damage to basal, epidermal keratinocytes [82].
The earliest changes can be seen in uninvolved and non-inflamed skin and are characterized with colloid body formation and pigmented macrophages in the dermis [83]. Colloid bodies (also known as Civatte bodies) are degenerated keratinocytes and electron microscopy has shown fibrillar degeneration of basal keratinocytes specifically [84, 85].
Classic changes are seen in established lesions with: ortho-hyperkeratosis, wedge-shaped hypergranulosis, saw-toothed rete ridges, epidermal hyperplasia, lymphocytes at the dermal-epidermal junction, Max Joseph spaces (focal, sub-epidermal clefts seen in 20 % of cases), squamatization (loss of maturation and flattening of the basal layer), and colloid bodies [86] (Fig. 31.8). LP is characterized by a dense, continuous, and band-like lympho-histiocytic infiltrate at the dermal-epidermal junction (DEJ). The heavy infiltrate can result in effacement of the DEJ. Parakeratosis and eosinophils are absent.
Fig. 31.8
Histology of classic cutaneous lichen planus (a) Left– Hematoxylin and Eosin (H&E) (40×) The characteristic findings of compact ortho-hyperkeratosis, wedge shaped hypergranulosis, sawtoothed rete ridges, and a lichenoid infiltrate. Small epidermal clefts (Max-Joseph space) can be seen centrally. (b) Right– (H&E 200×) Dense, lichenoid lymphocytic infiltrate with scattered apoptotic keratinocytes and pigment incontinence (Courtesy of David J DiCaudo MD)
Late disease is characterized by: atrophic epidermis, effacement of the rete ridges, occasional colloid bodies, dermal fibrosis, and melanophages. When few colloid bodies are present, distinguishing from poikiloderma may be very difficult.
Hypertrophic LP is characterized by: hyperkeratosis, acanthosis, papillomatosis, and thickened collagen bundles in the dermis. Hypertrophic LP can be mistaken for squamous cell carcinoma; therefore, good clinical pathological correlation is needed to avoid inappropriate treatment [87]. Eosinophils are more commonly seen in hypertrophic lesions [88]. Mucosal lesions tend to have less specific changes and genital disease can often be inconclusive. Parakeratosis and an absent granular layer are common at mucosal sites.
LPP is characterized by a perifollicular, lymphohistiocytic inflammatory reaction with perifollicular fibrosis, scarring, and follicular atrophy. Initial inflammation is at the level of the isthmus and infundibulum and spares the lower segment [45]. Permanent hair loss likely results from damage to the stem cells in the bulge and subsequent fibrosis [89].
LDEs may be indistinguishable from LP. However, if present, atypical features like parakeratosis, eosinophils (seen in up to two-thirds of cases), plasma cells, large numbers of apoptotic keratinocytes, and perivascular lymphocytes extending into the reticular dermis may aid in the diagnosis [90, 91]. In one study, focal parakeratosis, focal clusters of colloid bodies in the granular layer and stratum corneum, and focal epidermal disruption were seen in 50 % of LDEs and no cases of LP [91]. Cluster of differentiation-8 (CD8) positive Granzyme B positive lymphocytes appear to predominate in LDE versus classic LP [90].
Immunofluorescence
In cases of LP with positive immunofluorescence, fibrin and IgM (bound to colloid bodies) are present in 100 % and 93–100 % of cases, respectively [83, 92] (Fig. 31.9). Shaggy fibrin is the most common finding and best predictor of LP and can be seen in early disease without a prominent inflammatory infiltrate. The criterion for LP requires basement membrane zone fibrinogen and colloid bodies with one or more conjugates (Mayo Clinic Criteria) [93]. Colloid bodies have a better predictive value in oral lesions. DIF of OLP (sensitivity of 61 % and specificity of 96 %) is inferior to both hematoxylin and eosin (H&E) (sensitivity of 84 % and specificity of 93 %) and clinical impression (sensitivity of 74 % and specificity of 87 %) [93]. These findings emphasize the importance of clinical examination and diagnosis in classic LP. DIF has a role in atypical disease as well as ulcerative and vesiculobullous variants.
Fig. 31.9
Immunofluorescence of lichen planus (a) Shaggy basement membrane zone for fibrinogen (b) Scattered and clumped cytoid bodies with Immunoglobulin M (IgM) (Courtesy of Michael J Camilleri MD)
Location of disease governs sensitivity of detection by DIF (in decreasing order): mouth floor, the ventral side of the tongue, superior labial mucosa, hard palate and buccal mucosa. The gingiva is the least sensitive location, although other studies refute this, and suggest the dorsal tongue [93, 94]. The optimal location for biopsy of cutaneous LP is on the proximal trunk with avoidance of the distal extremities [92]. A biopsy of lesional tissues for DIF can yield false negatives since immune deposits are degraded by intense inflammation or damage in the basal membrane zone.
Traditionally, biopsies have been taken from perilesional skin; however, more recent data, in OLP, suggests the same diagnostic yield of more distant biopsies (greater than 1 cm from the lesion) [94, 95]. Splitting of biopsy samples is common in oral disease; however, the sensitivity is significantly less on split samples (40 % versus 65 %) [94]. Subsequent studies of mucosal and glaborous skin showed no difference in sensitivity and specificity of DIF [92].
On DIF, there can be considerable overlap between LP and LE with the majority of cases of LE showing immune deposition on colloid bodies and fibrin at the DEJ. The clustering of colloid bodies is much more common in LP. Multiple immunoglobulin (IgG, A, and M) conjugates and granular, basilar deposition of Igs are more common in LE, and the diagnosis should be suspect when present in LP [96].
Differential Diagnosis
The differential diagnosis of LP is quite broad. A more practical approach is to look at the age of the individual, morphology of the primary lesion, and site of involvement (Table 31.2).
Table 31.2
Differential diagnosis of lichen planus
Morphology and age: |
Classic: Psoriasis, Lichenoid drug, Lichen simplex chronicus, Chronic cutaneous lupus, Graft versus host disease, Secondary syphilis, Pityriasis rosea, Mycosis fungoides |
Annular: Granuloma annulare, Tinea corporis |
Linear: Lichen striatus, Linear epidermal nevus, Psoriasis, Darier’s disease |
Hypertrophic: Lichen simplex chronicus, Prurigo nodularis, Lichen amyloidosis, Kaposi sarcoma, Squamous cell carcinoma, Psoriasis |
Atrophic: Lichen sclerosus, Cutaneous lupus erythematosus, Poikiloderma |
Vesiculobullous: Lichen planus pemphigoides, Epidermolysis bullosa pruriginosa, Pemphigus vulgaris, Bullous pemphigoid, Bullous amyloidosis |
Follicular: Lichen nitidus, Lichen spinulosa |
Childhood: Lichen nitidus, Lichen striatus, Pityriasis lichenoides, Papular acrodermatitis of childhood |
Special site: |
Nail: Psoriasis, Onychomycosis, Alopecia areata |
Genital: Psoriasis, Seborrheic dermatitis, Fixed drug eruption |
Palms and soles: Secondary syphilis, Erythema multiforme |
Scalp: Cicatricial alopecia, Lupus erythematosus, Inflammatory folliculitis, Alopecia areata, Cicatricial pemphigoid, Keratosis follicularis spinulosa decalvans |
Mucosal: Paraneoplastic autoimmune multi-organ syndrome/Paraneoplastic pemphigus, Candidiasis, Lupus erythematosus, Leukokeratosis, Secondary syphilis, Traumatic patches, Chronic ulcerative stomatitis, Erythema multiforme |
Histological: |
Lichenoid keratosis, Poikiloderma, Chronic cutaneous lupus erythematosus, Fixed drug eruption, Lichen nitidus, Lichen striatus, Lichenoid drug, Graft versus host disease, Mycosis fungoides, Contact dermatitis, Keratosis lichenoides chronica, Erythema dyschromicum perstans, Lichenoid and granulomatous dermatitis |
Prognosis
Most cutaneous LP resolves within 1–2 years. Disease duration, in ascending order, is: generalized cutaneous, non-generalized cutaneous, cutaneous and mucosal, mucosal, hypertrophic, and LPP [97]. Recurrence is seen in up to 20 % of cases but is more common in generalized cutaneous disease [11, 98]. In higher Fitzpatrick skin types, post-inflammatory changes manifest as significant, persistent pigmentary abnormalities.
Pathogenesis
The pathogenesis of LP is unknown. Many contributing factors are implicated and include, infectious, autoimmune, metabolic, psychosomatic, and genetic causes. The initial theories of LP, described by Sabouraud in 1910, emphasized a dermally based process with secondary involvement of the basal cells of the epidermis [99]. Thyresson and Moberger challenged this concept and proposed that LP was a process focused at the DEJ [84]. Black provided evidence of decreased respiratory enzyme activity in the epidermal cells as a possible early driver of LP [100]. However, the changes seen may have been a secondary phenomenon to the basal damage. The basal keratinocyte damage was thought to be secondary to targeted cell mediated immune (CMI) mechanisms, but the exact pathogenesis remained largely illusive [101].
Shiohara et al. further described the T-cell mediated attack upon the epidermis and re-focused attention to CMI and away from secondary humoral mediated processes [102]. Immune complexes have been found to down regulate the ability of macrophages to present antigen as well as stimulate a cytotoxic response [103, 104]. CD4-positive T-helper (CD4-Th) cells persistent in the dermis despite disease chronicity, and CD8-positive T-cytotoxic (CD8-Tc) cells have been found in close proximity to damaged basal keratinocytes in conjunction with exocytosis [105].
Modern theories encompass three major stages: antigen recognition, lymphocyte activation, and keratinocyte apoptosis. A fourth stage, resolution, is a new and emerging topic and will be discussed briefly. Research on LP often separates oral and cutaneous disease. However, the major mechanisms underlying disease subtypes are likely the same, although mechanisms targeting specific epithelial sites are enigmatic. A unified theory of LP does not exist; however, we present the modern view of the topic (Fig. 31.10).
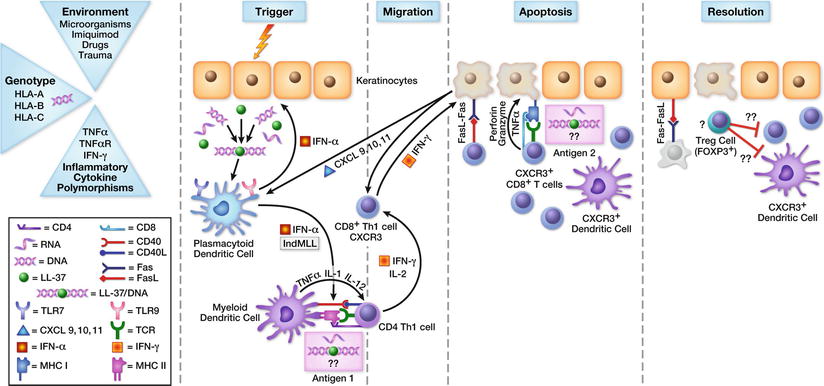
Fig. 31.10
Immunopathogenesis of lichen planus. The occurrence of triggering factors in a genetically predisposed individual carrying LP-associated genes, results in disease development. During the initiation phase, damage to keratinocytes results in the release of deoxyribonucleic acid (DNA), ribonucleic acid (RNA), and cathelcidin (LL37). These proteins stimulate plasmacytoid dendritic cells (PDC) via toll like receptors (TLR)-7,-9 which result in the release of interferon alpha (IFN-α). IFN-α can have both local and distant affects upon myeloid dendritic cells (MDC) as well as keratinocytes. Stimulated MDC will interact with CD4-Th cells with the correct antigen. The antigen remains unknown but may represent a viral derived peptide. MDC will stimulate CD4-Th cells via the release of TNF-α, Interleukin (IL) -1, and −12. In addition, CD40 and CD40 ligand (CD40L) will result in the co-stimulation of the CD4-Th/MDC interaction. Stimulated CD4-Th cells then release IFN-γ and IL-2. These cytokines stimulate CD8-Tc cells. The stimulated CD8-Tc cells expressing Chemokine receptor-3 (CXCR-3) will migrate to the DEJ following the release of chemokine ligands (CXCL) −9, −10,−11. These chemokines are released by stressed and stimulated keratinocytes. The stimulated CD8-Tc cells will interact with the stressed keratinocytes and can induce apoptosis with the proper signaling receptors. This antigen also remains unknown but may be a self-antigen released by local stress. The major kill signals are TNF-α, granzyme, and perforin. Fas and Fas ligand (Fas-L) are expressed on both keratinocytes and lymphocytes. Therefore, the Fas -Fas-L interaction is likely involved in both apoptosis as well as disease resolution. Local CXCR-3+ DC and T-regulatory (T-reg) cells may also modulate the LTR
The Cellular Immune Response
Antigen Recognition
The predominate cell mediating LP is the CD8-Tc cell. The targeted antigen(s) and or trigger(s) for LP remain unknown. However, in other diseases like lichenoid graft versus host disease (GVHD), the target antigens are the alloantigens. In oral disease, a LP-specific antigen associated with major histocompatibility complex (MHC) class I on keratinocytes has been reported [106]. It remains to be established if this antigen is an auto-reactive peptide or an exogeneous antigen. Circulating antibodies have been identified in multiple studies without a clear target antigen [83, 107]. The adaptive immune response is triggered by a “foreign” stimulus, and CD 56-positive CD 16-negative natural killer (NK) cells are recruited [108]. These cells are found in early lesions, express chemokine receptor-3 (CXCR-3), chemokine (c-c) motif ligand (CCL) -5, −6, and release IFN-γ and TNF-α [108]. NK cells may play a role in early propagation of LP.
The role of CD4-Th cells has come into focus in recent years. The CD4-Th population tends to be localized to the dermis with scattered cells in the epidermis. The level of CD4-Th cells correlates with the number of Langerhans cells (LC). LCs, one of the principal antigen-presenting cells of skin, upregulate MHC class II receptors in lichenoid disease [109]. In particular, the CD4-positive LC is seen in close approximation with the HLA-DR positive keratinocytes [110]. In addition, the CD4-Th cells have restricted V-beta gene expression, which suggests antigen specific oligoclonal T-cell expansion [111, 112]. Upon co-stimulation, these cells release large amounts of inflammatory cytokines including IFN-γ [113]. Taken together, these findings suggest an integral role of Langerhans cells, keratinocytes, and CD4 T helper cells in antigen presentation as well as propagation of the Th1 response via the production of IFN-γ.
The exact roles of exogenous and endogenous antigens in development of LP remain unknown. However, many drugs (see section “Drug-Induced Lichen Planus”), infections (see section “Infections”), contact allergens, and ultraviolet radiation (seen in LE) have been implicated [114–117]. With oral contactants, it has been debated if there is a bonafide hapten reaction or simply chronic inflammation, which manifests as a LTR. With the expanding use of biologics and inevitable adverse reactions, particularly TNF-α inhibitors, specifically LDE, imbalance and upregulation of type I IFN have been implicated in disease pathogenesis [118, 119]. This further substantiates previous reports of development of LP with therapeutic use of IFNs [120].
Lymphocyte Activation
Following antigen recognition, CD8-Tc cells are activated and undergo oligo-clonal expansion (outlined above). A cascade of both pro- and anti-inflammatory cytokines is released including: IL-2, −4, −10, IFN-γ, TNF-α, and transforming growth factor beta 1 (TGF-β1) [121, 122]. In LP, the balance between lymphocyte activation, down regulation, and the cytokine milieu may well determine the disease phenotype.
IFN-γ plays a central role in LP [123]. IFN-γ induces the expression of inflammatory chemokines such as chemokine ligand (CXCL)-9, −10, and −11 [123–125]. CXCR-3, their matching receptor, is predominantly expressed on the surface of IFN-γ-producing CD4-Th cells [124–127]. Peroxisome proliferated-activated receptor (PPAR) gamma inhibits CXCL-10 and −11 and its loss can result in scarring alopecia [128, 129]. IFN-γ increases peripheral blood mononuclear cell (PBMC) binding to HLA-DR positive keratinocytes [124]. However, blockade of the HLA-DR does not inhibit the interaction and lymphocyte function associated antigen-1 (LFA-1) is implicated in the interaction as it is reversed by neutralizing antibody [125]. LFA-1 is expressed on lymphocytes and interacts with intercellular adhesion molecule-1 (ICAM1) [130]. ICAM1 and vascular cell adhesion molecule (VCAM) expression is also enhanced by IFN-γ [126]. Mice pretreated with IFN-γ prior to transfer of T-helper cells exhibited a more brisk LTR but it was unchanged by pretreatment with TNF-α [127]. Therefore, IFN-γ is fundamentally involved in the upregulation of cellular adhesion molecules and the migration of lymphocytes to the DEJ [131, 132].
Keratinocyte Apoptosis
CD8-Tc cells are likely the terminal effector cells in LP. They have been found to co-localize with apoptotic keratinocytes and to have in-vitro cytotoxic activity against autologous keratinocytes [106, 133]. The cytotoxic effects of the CD8 positive cells can be inhibited by blockade of the MHC class I domain [106]. In addition to cytotoxic effects, lymphocytes in LP may be resistant to apoptosis suggested by increased levels of B-cell lymphoma-2 (Bcl-2) [134]. The markers of apoptosis include Caspase-3 and Bcl-associated X (BAX) expression. These proteins are elevated in LP in the basal and suprabasilar epidermis, respectively [134].
The exact mechanism of apoptosis in LP remains unknown. The possible mechanisms include: granzyme-B release, TNF-α-TNF-α R1 receptor interaction, and Fas-Fas-L interaction. Granzyme-B and granulysin are expressed at 100–200 fold higher levels in LP relative to normal skin [135]. Granzyme B, excreted by CD8-Tc cells, activates caspase-3 and likely promotes apoptosis in LP [136]. TNF-α upregulates the expression of matrix metalloproteinase-9 (MMP-9) in lesional T lymphocytes of OLP and has little effect upon the tissue inhibitor of metalloproteases (TIMPs) [137]. This likely leads to disruption of the basement membrane and damage to basilar keratinocytes. MMP-9 levels correlate with the phenotype, with higher lesional levels of messenger ribonucleic acid (mRNA) expression being associated with oral ulcerative disease [138]. MMP-9 is also involved in terminal differentiation and apoptosis of keratinocytes [139]. Taken together, MMP-9 likely disrupts the basement membrane homeostasis, blocking normal cell survival signaling and leads to apoptosis and cell death. Fas-Fas-L expression is elevated in OLP, correlates with disease progression, and likely contributes to apoptosis of keratinocytes [140–142].
Resolution
LP tends to be a self-resolving disease; however, there is a paucity of research into the resolution phase of disease. T-Regulatory (T-reg) cells are seen in OLP and correlates with disease subtype and activity [143, 144]. In vivo research in acute GVHD has shown the key role that T-reg cells play in the disruption of DC and allogeneic T-cell interactions [145]. DCs in LP have also been found to play a key role in T-cell migration [146]. However, DCs role is likely more complex as higher levels inversely correlate with the inflammatory infiltrate [147]. Fas-L, granzyme-B, and perforin can be expressed by keratinocytes allowing for apoptosis of lymphocytes [148, 149].
Genes and Gene Expression
Teleologically, immune system targeting of various naturally occurring but potentially deleterious antigens i.e., viruses and bacteria (see section “Toll-Like Receptors”), malignant cells, and exogenous contactants has potential benefit to the organism [150]. However, the generation of an immune response to exogenous antigens poses risk in the development of cross-reactivity to self-antigens or antigen mimicry and potential for cross-presentation [151, 152].
Genetic polymorphisms have been implicated in the risk of development of LP including: HLA, immune signaling molecules and receptors, and other polymorphisms, but their exact roles remain unknown. Copeman found HLA-B7 in 80 % of individuals with familial LP; however, further studies found HLA-B7 to be in 0–50 % of cases [15, 153–155]. Additional HLA types associated with familial and non-familial LP include: HLA-A3, −Aw19, −B18, −Cw8, −DR1, −DRB1*0101, −DQ1, −DQB1*0201 [32, 97]. The mode of inheritance appears to be autosomal dominant with variable penetrance. A study of OLP, in a Chinese family, found chromosome 3p14-3q13 as the candidate gene region for OLP [156].
Polymorphisms have been reported in immune related genes: IFN-γ, TNF-α, TNF-α R2, IL-4, −6, and −18 [32]. Polymorphisms in other genes include those involved in oxidative stress, prostaglandin-E2 (PGE2) synthesis, formation of transglutaminase, thyroid hormone synthesis, prothrombin, nuclear factor kappa-light-chain-enhancer of activated B cell (NFkB) as well as epigenetic regulation of genes by micro-RNA (miRNA)-146a and −155 [32] These polymorphisms may regulate increased activity of pro-inflammatory mediators as well as dysfunctional proteins and aberrant signaling. Gene expression profiling of LP, compared to atopic dermatitis and psoriasis, identified expression of the CXCR-3 ligand, CXCL-9, as the most specific marker for LP [157]. In addition, keratinocytes were confirmed as the source of type I IFNs (−α & -β) [157]. Future research using large, case-control genome-wide array studies, as was done with psoriasis, may clarify the current risk alleles and identify additional risk alleles for LP [158].
Cellular Immune Response
Dendritic Cells
Dendritic cells (DCs) play a key role in antigenic stimulation of naïve T-cells. Three major dendritic cell populations are involved in development of LP, including LCs (CD1a +, Langerin +), dendritic cell-specific intercellular adhesion molecule-3 grabbing non-integrin positive DCs (DC-SIGN DCs), and plasmacytoid DCs (PDC) (CD-123+, BDCA+) [159]. DCs are the primary antigen presenting cells and are involved in antigen processing as well as presentation to T-cells [160]. When DCs encounter an antigen, they undergo maturation, resulting in specific acquisition of phenotypic properties, including CCR7 expression, adhesion, and co-stimulatory marker expression, which induce nodal homing and T-cell stimulation [161, 162].
Langerhans Cells
LCs express: CD1a, Langerin, and E-cadherin, and are usually located in the suprabasal layer of the epidermis [163]. In LP, LCs are critical in the epidermal migration of T-cells. LCs present autoantigens or foreign antigens to T-cells, which can activate T-cells. Upon activation, LCs downregulate Langerin and E-cadherin as well as upregulate CD80 and 86, which enhances T-cell stimulation [164]. Over time, the LCs migrate towards the basal epidermis [165].
The exact role of LCs remains unknown, though they likely play integral roles in both promoting and regulating the inflammatory response. Mouse models show that the migration of T-cells can be impaired with tape-stripping of the skin (95 % of LCs removed) [146]. In OLP the number of LCs inversely correlates with the number of inflammatory cells [147]. The paradoxical findings related to DCs may eventually be reconciled by the intricate balance of deletion of autoreactive populations versus potential propagation of autoimmunity, which may not be mutually exclusive [166].
DC-SIGN Dendritic Cells
The role of DC-SIGN DCs is unknown in LP. Interstitial DCs do not express langerin but do express DC-SIGN, which binds to ICAM2 and −3 and allows for extravasation as well as interaction of DCs and naïve T-cells [167–170]. DC-SIGN DCs have pluripotent differentiation in that one population stimulates T-cells and another is macrophage-like, which lack T-cell stimulatory function and can stimulate B cells [171].
Plasmacytoid Dendritic Cells
PDCs express CD68, cutaneous lymphocyte-associated antigen (CLA), IL-3Rα (CD-123) and blood dendritic cell antigen-2 (BDCA2), but lack expression of CD11c [172]. PDCs are found in the dermis and are likely responsible for the maturation of DCs and play a central role in the amplification of cytotoxicity in lymphoid cells. Upon stimulation, PDCs upregulate CD40-L, express IL-12, and type I IFN, which stimulate a Th1 response [172]. With maturation, PDCs downregulate CXCR-3 and L-selectin, which allows for migration from the epidermis into the stroma, lymphatics, and eventually the lymph nodes [172, 173].
PDCs have the unique capacity to rapidly produce large amounts of interferon- α (IFN-α) upon recognition of viral RNA and deoxyribonucleic acid (DNA) through TLR7 and −9, respectively [174]. Type I IFN producing PDCs recruit CD8-Tc cells, carrying CXCR-3 ligands in their granules, via CXCR-3–CXCL-10 interaction, which represents an important amplification step in LP [150, 175]. In addition, PDCs express CXCR-3, which allows for migration, amplification, and modulation of the local LTR [175].
PDCs are normally unable to respond to self-nucleic acids; however, in cutaneous LE PDCs become activated to produce type I IFNs by self-nucleic acids in complex with antibodies to DNA or nucleoproteins [176–178]. Type I IFN results in the maturation of MDCs, DC-SIGN DCs and LCs, and increases MDCs’ ability to stimulate T-cells, which can result in auto-reactive immune events [179]. It remains speculative whether these triggers exist in LP.
T-Cells
Both cytotoxic and helper T-lymphocytes play central roles in LP as described earlier (see section, “Antigen Recognition,” “Lymphocyte Activation,” “Keratinocyte Apoptosis,” and “Resolution”). The role of T-Reg cells also remains speculative but their general mechanisms of activity are discussed below.
T-Regulatory Cells
Foxp3-positive CD4-positive CD25-positive regulatory T cells (T-Regs) are critical for the regulation of host tolerance and suppression of pathological immune responses. T-Reg cells can be readily identified in the skin; however, no significant differences were found between normal skin and many inflammatory dermatoses, including LP [180]. Recently, T-reg cells and the inducers and signaling molecules, TGF-β and IL-10, were found to be upregulated in OLP and were diminished after effective treatment [181]. This suggests a role for T-Regs, induced by IL-2 and TGFβ, as well as synthesis of IL-10 and TGF-β in the resolution of LP [182, 183]. Human anti-inflammatory macrophages (m2 type) induce T-Reg cells and may also play a role in disease resolution [184].
Polymorphisms in specific cytokines, and receptors, as well as pathways in the generation of suppressive immune cells may lead to a prolonged or inappropriate inflammatory response. Genetically altered mice with autoreactive CD8+ T cells do not develop toxic epidermal necrolysis, a severe, necrotic form of interface dermatitis, until they are depleted of T-Reg cells [185]. Taken together, T-Reg cells are involved in attenuating the immune response and are diminished in cutaneous LE and other LTR, but their role in propagation and clearance of LP has yet to be clearly defined [186].
CXCR-3 Ligands
CXCR-3 ligands, CXCL9, −10, −11, are required in the recruitment of CD8-Tc cells as well as PDCs in LTR [188]. CD8-Tc cells harbor CCL5 and CXCR10 in their granules, which suggest auto-inductive and propagating pathways of activation [188]. CXCL-12 is homeostatic in nature, has an unclear role in LP, but is upregulated in oral disease [189]. The upregulation of inflammatory and homeostatic chemokines results in the recruitment of memory T cells [114, 190]. IFN-γ and TNF-α stimulate keratinocytes to release CXCR-3 ligands [123, 191]. These ligands are upregulated in LP relative to other inflammatory skin diseases [157]. CXCR-3 positive CD8-Tc cells as well as PDCs have a high affinity for CXCR-3 ligands that facilitate migration and recruitment at the DEJ with subsequent basement membrane disruption [175, 190, 192]. Similar mechanisms, although mediated by different stimuli, have been described in cutaneous LE, and lichenoid GVHD [114, 192].
Interferon-α
IFN-α is produced primarily by PDCs and is a critical mediator in DC maturation (see section “Dendritic Cells”), as well as the amplification and the recruitment of CD8-Tc cells [150] IFN-α is a potent mediator of the expression of CXCR-3 ligands. IFN-α rapidly induces CXCL-9, −10, −11, and −12 expression in primary keratinocytes, dermal fibroblasts, and dermal endothelial cells. The upregulation of CXCL-12 in conjuction with the CXCR-3 ligands suggests that IFN-α plays a key role in PDC recruitment as well as CD8-Tc cells and memory T cells. T-lymphocyte recruitment produces IFN-γ, which results in an amplification loop.
Interferon-γ
IFN-γ plays a central role in CMI and is over-expressed in lesional LP (see section “Lymphocyte Activation”) [189, 193]. Upregulation of IFN-γ has been identified in keratinocytes as well as cytotoxic T cells of LP [113]. IFN-γ induces expression of Fas on keratinocytes contributing to apoptosis [194].
Toll-Like Receptors
TLRs are part of the innate immune response, which recognize specific molecular components conserved among microorganisms [195]. TLRs induce an innate inflammatory response and mediate antigen-specific adaptive immunity [195].
PDC are likely activated by TLR7 and −9 (see section “Dendritic Cells”). While specific triggers of LP are unknown, human herpes virus type 7 (HHV7) in LP has been found to co-localize with PDCs [115–117]. Though not conclusively confirmed, this suggests that viral DNA in conjunction with TLR9 may activate PDCs in early lesions of LP [115–117]. Increased expression of TLR9 has been demonstrated in both oral and cutaneous LP [196, 197]. Similarly, imiquimod, an inducer of TLR7, is reported to cause LP [198–200].
Koebnerization, disease triggered by local skin injury, may be induced by cathelcidin (LL37), an endogenous antimicrobial peptide, which can bind to self-DNA. While this has not been observed in LP, activation of PDCs by LL37 bound to self-DNA has been shown in psoriasis [201]. Meller has suggested that a similar mechanism may occur in an individual with a different genetic predisposition [122]. TLR2, which drives a humoral-mediated immune response, is downregulated in OLP while TLR4, which drives a CMI response, is upregulated in OLP [202]. TLR3 polymorphism has been associated with an increased risk in developing OLP as well as being a risk factor for poor survival in oral cancer [203, 204]. Taken together, there is an integral role between the host-microbial response in OLP and likely in cutaneous LP as well.
Treatment
The treatment of LP is challenging for both physicians as well as patients. Due to its ability to affect multiple ectodermally derived tissues, LP often requires a multidisciplinary approach with dermatologists, dentists, and gynecologists. The goal of therapy is to minimize morbidity and improve the patient’s quality of life.
The basic concepts in the treatment of LP have remained largely unchanged over the last decade. The therapies are mainly divided into skin directed and systemic agents. The therapies for various ectodermal tissues are also similar. Nearly all of these agents act in a manner to depress the immune response. To date, there are not disease specific medications for LP. However, Janus Kinase (JAK) inhibitors target CD8-Tc cells and represent a potential, disease-specific treatment of lichenoid diseases, including LP [205]. This section will provide a brief overview of the general approach to therapy for LP; however, emphasis will be placed upon unique treatments for variants of LP and their potential pharmacological targets.
Cutaneous Lichen Planus
Topical Corticosteroids
Despite few clinical trials, high potency topical corticosteroids are considered first-line therapy for limited cutaneous LP. Occlusion may be necessary to increase penetration in cases of hypertrophic LP. The sole randomized controlled trial comparing calcipotriene to betamethasone valerate (twice daily for 12 weeks) found no difference between treatments [206]. If no response is observed to twice daily application for 2–4 weeks, changing to a higher potency corticosteroid or intralesional injections should be considered [207].
Topical Calcineurin Inhibitors
There are no trials using topical calcineurin inhibitors (TCIs) in cutaneous LP. However, clinical data in OLP suggests that topical TCIs are likely the most effective topical therapy for LP. Application of tacrolimus 0.1 % ointment is as effective as 0.05 % clobetasol [208].
Intralesional and Systemic Corticosteroids
Intralesional corticosteroids (5–10 mg/mL injected on a monthly basis) can be highly effective in resistant and hypertrophic LP. However, one should use caution to prevent excessive trauma to avoid Koebnerization. Systemic corticosteroids for cutaneous LP have only been reported in one study with a 90 % response rate and 32 % relapse rate at 6 months [209]. In our clinical experience, systemic corticosteroids are highly effective but are associated with high rates of relapse upon discontinuation. Therefore, oral and intralesional therapy should always be combined with topical therapy.
Phototherapy
Phototherapy has been used successfully in many inflammatory diseases of the skin. Ultraviolet-B (UVB) exposure of DCs results in impaired DC-CD4-Th cell interaction that culminates with T-cell apoptosis [210]. In addition, phototherapy alters cytokine expression, which suppresses CD8-Tc cells [211]. UVB (three times weekly until remission with taper after remission over 3–6 weeks) has a 70 % remission rate and 85 % of those patients remained in remission at 34 months [212]. Narrowband UVB (311 nm) is as effective in LP and has largely supplanted Ultraviolet-A (UVA), psoralen plus UVA (PUVA), and UVB phototherapy [213].
Miscellaneous
The mechanism of action of metronidazole in LP is unknown but may be mediated by its antimicrobial activity as well as immunosuppressive effects on human blood lymphocytes [214]. An open labeled study of oral metronidazole (250 mg three times daily for 12 weeks) showed a 74 % response rate at 3 months of follow up [215]. Alternate dosing (500 mg twice daily for 20–60 days) has also been reported to be successful [216]. Due to its side effect profile, metronidazole is often considered first line; however, one should caution patients as well as monitor for possible sensory peripheral neuropathy [217].
Sulfasalazine (initial dose 1 g daily with an increase every 3 days by 0.5 g to a max of 2.5 g daily) has the highest level of evidence of efficacy for LP with an 83 % improvement in skin lesions and a 91 % improvement in itch at 6 weeks in the therapy group [218, 219]. Sulfasalazine likely downregulates the expression of ICAM1, decreases leukotriene synthesis, and decreases the number of lesional T lymphocytes [220].
A double blind, placebo control trial of acetretin (30 mg daily for 8 weeks) showed marked improvement in 64 % of individuals [221]. Mucocutaneous side effects and hyperlipidemia were common. Retinoids may have activity by downregulating VCAM1 on endothelial cells and modulation of cyclooxygenase-2 (COX2) and TNF-α preventing the homing of lymphocytes to the skin and stimulation of the inflammatory cascade [222, 223].
Methotrexate has been shown to be of benefit for more recalcitrant disease as well as in specific forms of disease, including hypertrophic LP and LPP. Methotrexate preferentially targets lymphocytes 1000-fold relative to keratinocytes and inhibits proliferation and has cytotoxic activity [224]. Recent, non-randomized, prospective data has shown methotrexate (15–20 mg weekly for 4–24 weeks) to be highly efficacious with complete responses in 58–91 % of cases [225–227].
Other therapies including: mycophenolate mofetil, cyclosporine, TNF-α inhibitors, trimethoprim-sulfamethoxazole, griseofulvin, itraconazole, terbinafine, antimalarials, tetracyclines, laser, IFN, allitretinoin, thalidomide, and low-dose heparin have also been reported.
Oral Lichen Planus
The cornerstone of treatment in OLP is good oral hygiene with regular professional dental cleanings [228]. Minimizing other exacerbating factors such as: contact allergens, drug reactions, reducing oral microbes, and minimizing trauma can reduce disease severity as well as frequency of flares. Replacement of dental amalgams and gold dental restorations can be beneficial, even in patients with negative patch testing [229, 230]. However, removal and restoration should be individualized based upon the severity of disease as well as the index of suspicion of the level of involvement of the metal or prosthesis.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


