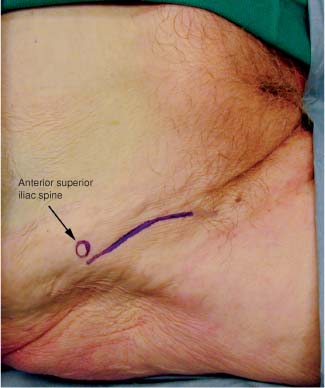
10 The lateral femoral cutaneous nerve, a nerve of the lumbar plexus, arises from the ventral rami of L2 and L3. It emerges from the lateral border of the psoas muscle and passes obliquely over the iliacus behind the parietal peritoneum (i.e., retroperitoneally) and iliac fascia (which it supplies) toward the anterior superior iliac spine. It enters the thigh still in a retroperitoneal position, passing through the lateral edge of the inguinal ligament just medial to the sartorius muscle attachment. The nerve passes through the proximal part of the sartorius and descends in the leg deep to the fascia lata. It gives off several small cutaneous branches before piercing the fascia ~10 cm below the inguinal ligament. The terminal branches of the nerve supply the skin and fascia on the anterolateral surfaces of the thigh between the levels of the greater femoral trochanter and the knee. Entrapment of this nerve causes the condition known as meralgia paresthetica.1 The first lumbar spinal nerve receives a fascicle from the subcostal nerve (T12) and divides into upper and lower branches. The upper branch then splits into the iliohypogastric and ilioinguinal nerves, whereas the lower branch joins a fascicle from the second lumbar spinal nerve to become the genitofemoral nerve. The subcostal nerve, iliohypogastric nerve, ilioinguinal nerve, and genitofemoral nerve travel within the posterior wall of the abdomen and pelvis in a course parallel to each other. The ilioinguinal nerve pierces the internal oblique muscle above the anterior part of the iliac crest and then runs above and parallel to the inguinal ligament to traverse the inguinal canal. The nerve emerges through the external ring to eventually supply the skin over the root of the penis, the adjoining part of the femoral triangle, and the upper part of the scrotum (mons pubis and adjacent part of the labium majoris in the female). The genitofemoral nerve penetrates the psoas major muscle and divides into genital and femoral branches. The genital branch passes through the inguinal canal and supplies the cremaster muscle and the skin of the scrotum in the male and the round ligament in the female. The femoral branch supplies sensation to the skin of the upper part of the femoral triangle. Either of these nerves can be injured in inguinal or femoral hernia repairs leaving the patient with disabling painful genital neuropathies.2,3 To expose the lateral femoral cutaneous nerve in the leg, the patient is placed in the supine position with the arms tucked to the side. The surgeon works from the ipsilateral side of the patient. For a more proximal, intrapelvic exposure see Chapter 8. The anterior superior iliac spine is marked and an incision is laid out that parallels the inguinal ligament for ~8 to 10 cm (Fig. 10-1). The skin is infiltrated with a 1% lidocaine with epinephrine solution in a 1:100,000 concentration. The skin and subcutaneous tissue are divided, and with blunt dissection the subcutaneous fat can be swept off the lateral portion of the inguinal ligament and its junction with the sartorius muscle (Fig. 10-2). The junction of the sartorius and the inguinal ligament forms an angle with its apex at the iliac spine. This landmark can be useful in locating the nerve, which courses through this angle. The fascia lata is then incised and retracted to reveal the surface of the sartorius muscle (Fig. 10-3). In the fat and fascia overlying the sartorius, or just medial to it, the nerve is located (Fig. 10-4). When the nerve is located, if necessary, the inguinal ligament may be divided to trace the nerve proximally (Fig. 10-5). To locate the ilioinguinal nerve the patient is placed in the supine position with the arms tucked at the side. The surgeon works from an ipsilateral position. The anterior superior iliac spine is marked and an incision that begins just medial to the spine and 2 to 3 cm superior to it is laid out. The incision travels obliquely in an inferomedial direction (Fig. 10-6). The skin is infiltrated with a 1% lidocaine with epinephrine solution in a 1:100,000 concentration. The skin and subcutaneous tissue are divided and with blunt dissection the fat is retracted to reveal the anterior rectus sheath medially and fibers of the external oblique laterally (Fig. 10-7). The rectus sheath medially and the external oblique laterally are divided in line with their fibers. The internal oblique muscle with the ilioinguinal nerve atop it is revealed (Fig. 10-8). The ilioinguinal nerve may then be isolated and traced distally and proximally as needed (Fig. 10-9).
LATERAL FEMORAL CUTANEOUS NERVE, ILIOINGUINAL NERVE, AND GENITOFEMORAL NERVE
ANATOMY
POSITIONING AND SURGICAL EXPOSURE
Lateral Femoral Cutaneous Nerve, Ilioinguinal Nerve, and Genitofemoral Nerve
Only gold members can continue reading. Log In or Register to continue







Full access? Get Clinical Tree


