 2 Laser treatment of vascular lesions
2 Laser treatment of vascular lesions
Summary and Key Features
• Vascular lesions are one of the most common indications for laser treatment
• Treatment of vascular lesions implements the theory of selective photothermolysis, confining thermal injury to the target of interest
• Pulsed dye laser remains the gold standard treatment for port-wine stains, and while most improve, the minority clear completely
• Early laser treatment improves port-wine stain response
• Alexandrite laser can be implemented for treatment of hypertrophic, or pulsed dye laser resistant, port-wine stains
• Indications for laser treatment of hemangiomas includes ulcerated lesions and involuted lesions with residual telangiectasias and / or textural change
• The role of laser treatment for proliferating hemangiomas remains less clear, and may be most beneficial for superficial hemangiomas
• Deeper-penetrating near-infrared lasers may be implemented to treat select venous malformations
• Vascular lasers and intense pulsed light are the treatment of choice for the background erythema and telangiectasias associated with rosacea
• Poikiloderma of Civatte can be successfully treated with intense pulsed light, or a combination of vascular and pigment selective lasers
Introduction and history
Three components are necessary for selective photothermolysis: (1) a laser wavelength with preferential absorption of the target chromophore, (2) appropriate pulse duration matched to the target size, and (3) a fluence that both treats the target and minimizes non-specific thermal related injury. The ideal pulse duration is equal to or somewhat shorter than the thermal relaxation time of the target vessel. The thermal relaxation time is defined as the time for 50% of the heat to dissipate from the target of interest. A pulse duration that is too short may not be effective, whereas one that is too long may cause heat to dissipate to surrounding structures and cause unwanted thermal injury. The classic target chromophore for vascular lesions has been oxyhemoglobin, which has the greatest absorption peaks at 418, 542, and 577 nm (Fig. 2.1). The laser light is absorbed by oxyhemoglobin, and converted to heat, which is transferred to the vessel wall causing coagulation and vessel closure. Other hemoglobin species have more recently been recognized as appropriate targets, depending on the vascular lesion. For example, venous lesions may benefit from wavelengths of light that target deoxyhemoglobin. The alexandrite laser at 755 nm is close to a deoxyhemoglobin absorption peak and has been used for refractory or hypertrophic PWS, a venocapillary malformation. Methemoglobin absorption has also been recognized as a potential target chromophore.
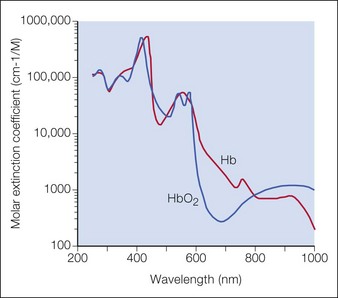
Figure 2.1 Optical absorption of hemoglobin.
Source: Dr Scott Prahl, http://omlc.ogi.edu/spectra/hemoglobin.
The most commonly used vascular lasers and light sources include:





Vascular anomalies classification
PWS, a type of capillary malformation, and hemangiomas are the two most common vascular anomalies that present for laser treatment (Table 2.1).
Table 2.1 Comparison of infantile hemangioma and port-wine stain
| Infantile hemangioma | Port-wine stain | |
|---|---|---|
| Onset | ||
| Course | ||
| Tissue marker |









Port-wine stain birthmarks
Overview
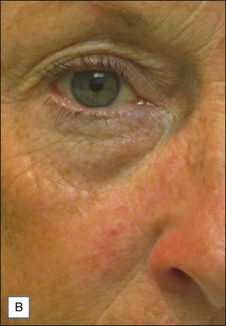
PWS are vascular malformations that are composed of ectatic capillaries and post-capillary venules in the superficial vascular plexus. PWS vessels are characterized by diminished vascular tone and decreased density of nerves, especially those with autonomic function. In most cases, PWS are congenital, though in rare cases they may be acquired. PWS are found in approximately 0.3% of newborns. They tend to occur on the head and neck, although they may appear anywhere on the body. PWS persist throughout life and many thicken with time (Fig. 2.2). Geronemus et al reported that the mean age of hypertrophy is 37 years and, by the fifth decade, approximately 65% of lesions had become hypertrophied or nodular. There may be associated soft tissue overgrowth, leading to functional impairment in areas such as the lip or eyelid. Vascular blebs often form and may bleed with minimal trauma. These lesions are often considered disfiguring and many patients or their families seek treatment. PWS vessels vary in size from 7–300 µm with older patients tending to have larger vessels.


Treatment
The PDL is the most commonly used laser to treat PWS. Treatments are typically done at 4–6 week intervals, and it is not uncommon for 10 or more treatments to be performed initially until a plateau is reached or the lesion clears (Fig. 2.3). Larger spot sizes allow for greater depth of penetration and so the clinician should select the largest spot size that will provide sufficient fluence to achieve the desired end point, while confining the treatment to the area of interest. It is advisable to determine the fluence threshold on the darkest portion of the PWS with 1 or 2 test pulses before treating the entire lesion. The fluence is adjusted to achieve the desired end point. For the PDL, the desired end point is immediate purpura. A confluent gray color signifies that the fluence is too high. A cookbook approach to treatment may result in complications.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


