Chapter 4 Laparoscopic Repair of Parastomal Hernias 
1 Clinical Anatomy
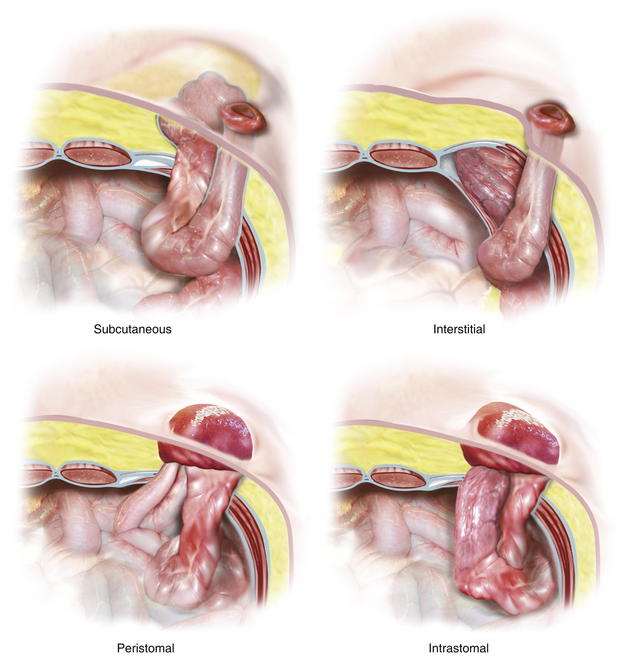
1 Types of Parastomal Hernias
Parastomal hernia has been anatomically classified into four subtypes: (Fig. 4-1)


2 Preoperative Considerations
 The life expectancy of the patient and any predisposing factors, such as malignancy and obesity, should influence the decision to proceed with surgery.
The life expectancy of the patient and any predisposing factors, such as malignancy and obesity, should influence the decision to proceed with surgery.
 CT scan is useful to delineate parastomal defects, any associated incisional hernia, and the content of the hernia (Fig. 4-2).
CT scan is useful to delineate parastomal defects, any associated incisional hernia, and the content of the hernia (Fig. 4-2).




3 Operative Steps
There are two techniques for laparoscopic repairs of parastomal hernias: the keyhole and the Sugarbaker techniques. Keyhole technique may be associated with bowel herniation between the mesh hole and the stoma loop. We have developed a technique that closes the gap between the mesh and the stoma loop and facilitates intracorporeal mesh manipulations (Scroll technique) during keyhole repairs. The Sugarbaker technique avoids the risk of herniation through the keyhole, but it does create an acute angle as the bowel exits the mesh and can cause obstruction (see Fig. 4-11). Meticulous attention to the details of mesh fixation and placement can limit these complications.
 1 Laparoscopic Parastomal Hernia Repair Technique: The Scroll Technique
1 Laparoscopic Parastomal Hernia Repair Technique: The Scroll Technique





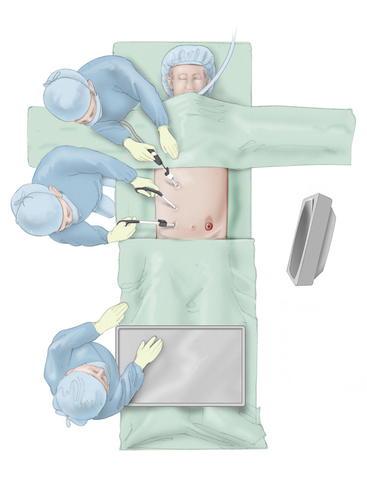
 Trocar Placement (Fig. 4-4)
Trocar Placement (Fig. 4-4)
 For a left lower quadrant stoma, an initial 12-mm Hasson trocar is placed in the right upper quadrant away from the hernia defect.
For a left lower quadrant stoma, an initial 12-mm Hasson trocar is placed in the right upper quadrant away from the hernia defect.







