Chapter 3 Laparoscopic Repair of Atypical Hernias
Suprapubic, Subxiphoid, and Lumbar 
1 Clinical Anatomy
 The laparoscopic repair of incisional hernias that occurs at the extremes of the abdomen either superiorly, inferiorly, or laterally can present many unique challenges to the surgeon. These hernias are often near major neurovascular or bony structures, making adequate overlap of mesh and fixation difficult. Typical locations for these types of hernias include the subxiphoid, suprapubic, or lumbar areas. These atypical hernias can often be approached and repaired laparoscopically with careful preoperative planning.
The laparoscopic repair of incisional hernias that occurs at the extremes of the abdomen either superiorly, inferiorly, or laterally can present many unique challenges to the surgeon. These hernias are often near major neurovascular or bony structures, making adequate overlap of mesh and fixation difficult. Typical locations for these types of hernias include the subxiphoid, suprapubic, or lumbar areas. These atypical hernias can often be approached and repaired laparoscopically with careful preoperative planning.1 Suprapubic Hernia
 Correct and timely identification of the key structures in the lower anterior abdominal wall is critical for the safe laparoscopic repair of suprapubic hernias (Fig. 3-1). A careful preperitoneal dissection provides the needed landmarks for appropriate fixation to lessen the chance of postoperative recurrence.
Correct and timely identification of the key structures in the lower anterior abdominal wall is critical for the safe laparoscopic repair of suprapubic hernias (Fig. 3-1). A careful preperitoneal dissection provides the needed landmarks for appropriate fixation to lessen the chance of postoperative recurrence.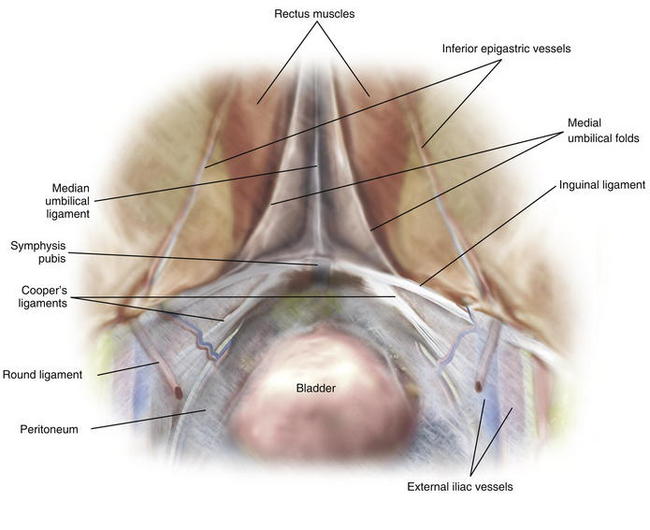
2 Subxiphoid Hernia
 Identification of the costal margins and xiphoid process provide the laparoscopic bounds of transabdominal fixation for repair of subxiphoid hernias (Fig. 3-2). Generous overlap of the mesh over the diaphragm helps provide adequate coverage of the fascial defect in lieu of superior fixation.
Identification of the costal margins and xiphoid process provide the laparoscopic bounds of transabdominal fixation for repair of subxiphoid hernias (Fig. 3-2). Generous overlap of the mesh over the diaphragm helps provide adequate coverage of the fascial defect in lieu of superior fixation.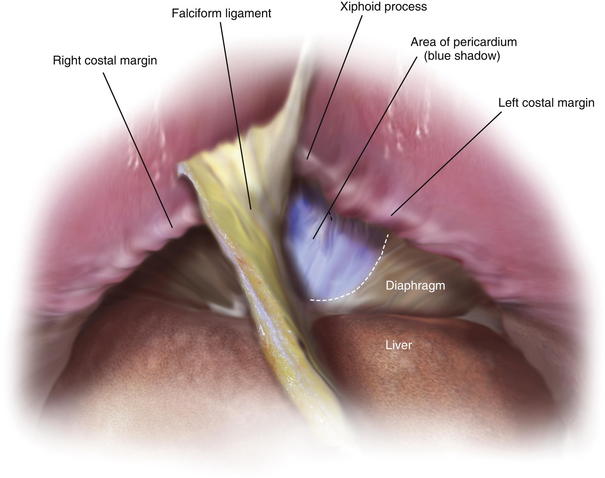
3 Lumbar Hernia
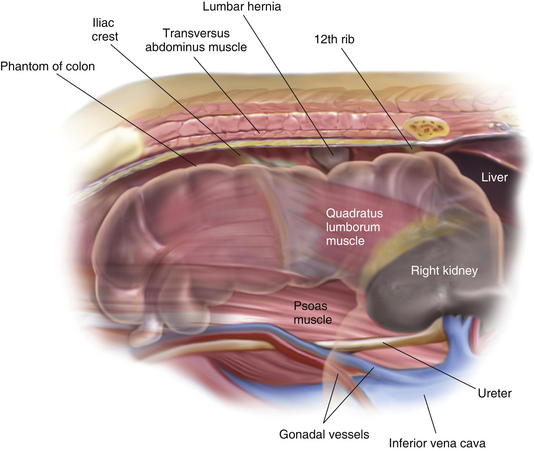
 The lumbar triangle is defined superiorly and laterally by the latissimus dorsi muscle, medially by the external oblique muscle, and inferiorly by the iliac crest (Fig. 3-3). Weakness of the internal oblique and transversus abdominis musculature within the lumbar triangle leads to hernia formation (Fig. 3-4). An anterior abdominal approach can be used for laparoscopic repair, with proper patient positioning used to strategically expose the lumbar triangle.
The lumbar triangle is defined superiorly and laterally by the latissimus dorsi muscle, medially by the external oblique muscle, and inferiorly by the iliac crest (Fig. 3-3). Weakness of the internal oblique and transversus abdominis musculature within the lumbar triangle leads to hernia formation (Fig. 3-4). An anterior abdominal approach can be used for laparoscopic repair, with proper patient positioning used to strategically expose the lumbar triangle.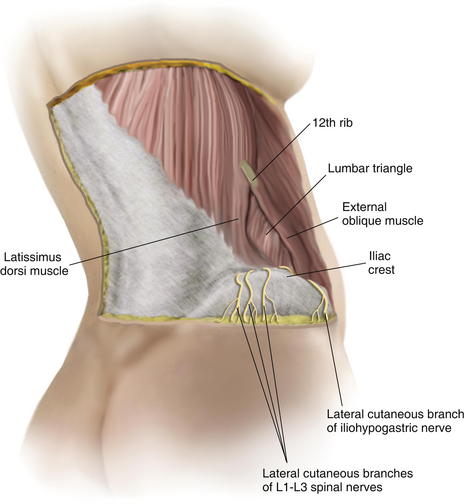
2 Preoperative Considerations
1 Laparoscopic or Open Approach?
 The decision to proceed between a laparoscopic or open approach to atypical hernias rests on the surgeon’s ability to estimate adequate coverage of the defect via laparoscopic approach and the candidacy of the patient for creation of a more physiologic repair via an open abdominal wall reconstruction. Relatively large fascial defects within 4 cm of the iliac crest are difficult to approach laparoscopically. Younger, active patients with sizable subxiphoid hernias may benefit from an open retrorectus or preperitoneal repair when dissection above the costal margins can be performed along with rectus medialization. Conversely, patients with smaller defects and those who may not tolerate an extensive abdominal wall reconstruction may benefit from a laparoscopic approach.
The decision to proceed between a laparoscopic or open approach to atypical hernias rests on the surgeon’s ability to estimate adequate coverage of the defect via laparoscopic approach and the candidacy of the patient for creation of a more physiologic repair via an open abdominal wall reconstruction. Relatively large fascial defects within 4 cm of the iliac crest are difficult to approach laparoscopically. Younger, active patients with sizable subxiphoid hernias may benefit from an open retrorectus or preperitoneal repair when dissection above the costal margins can be performed along with rectus medialization. Conversely, patients with smaller defects and those who may not tolerate an extensive abdominal wall reconstruction may benefit from a laparoscopic approach.2 Patient Positioning and Trocar Placement
 For laparoscopic suprapubic and subxiphoid hernia repairs, the patient is placed in the supine position, with arms tucked and carefully padded. Laparoscopic lumbar hernia repair often requires elevation of the ipsilateral side for posterior transabdominal fixation (Fig. 3-5). Usual trocar placement for laparoscopic ventral hernia repair should suffice for initial approach and lysis of adhesions (see Chapter 2, Fig. 2-3). These parts are placed more medially than usual on the contralateral side of the hernia defect. Access to the suprapubic region and myopectineal orifice is facilitated through three trocars at the level of the umbilicus; two are placed just lateral to the linea semilunaris, and one is placed at the umbilicus.
For laparoscopic suprapubic and subxiphoid hernia repairs, the patient is placed in the supine position, with arms tucked and carefully padded. Laparoscopic lumbar hernia repair often requires elevation of the ipsilateral side for posterior transabdominal fixation (Fig. 3-5). Usual trocar placement for laparoscopic ventral hernia repair should suffice for initial approach and lysis of adhesions (see Chapter 2, Fig. 2-3). These parts are placed more medially than usual on the contralateral side of the hernia defect. Access to the suprapubic region and myopectineal orifice is facilitated through three trocars at the level of the umbilicus; two are placed just lateral to the linea semilunaris, and one is placed at the umbilicus.Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


