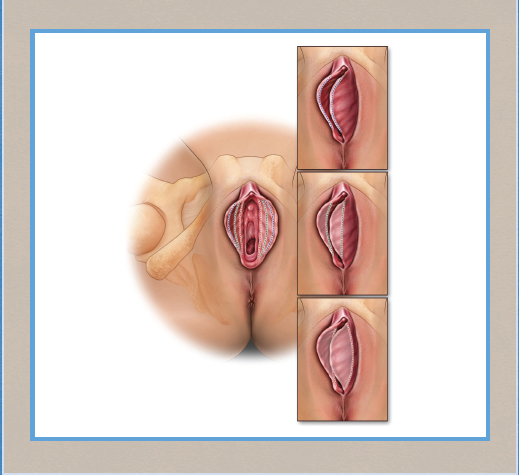
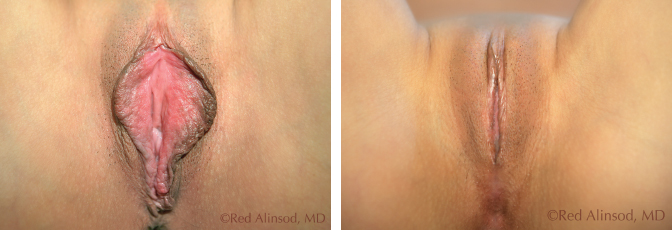
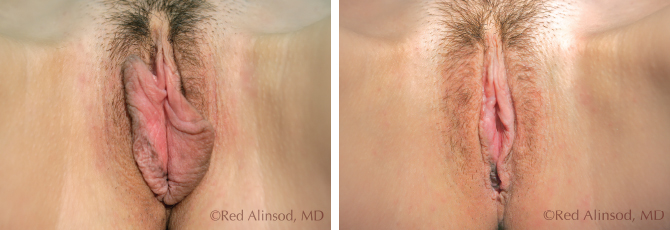
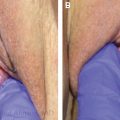
CHAPTER 5 • Most gynecologists who perform labiaplasty surgery use curved linear resection. In a survey of plastic surgeons who performed labia minoraplasties, the most commonly performed technique was curved linear resection (52.7%) followed by central V-wedge resection (36.1%).1 • Although the edge excision technique reportedly has fewer wound-healing complications, it leaves a suture line at the periphery that may rarely result in scar contracture and rare chronic pain during coitus.2 Wedge excisions leave the same type of scar but in a mostly horizontal manner. Scars causing pain are exceptionally rare, because labial scars dramatically diminish and soften and are generally not detectable within 6 months for both wedge excisions and linear excisions. • Different techniques may be preferable for different patients, depending on the advantages and disadvantages of the procedure, the degree and location of labia minora hypertrophy, and the patient’s cosmetic preference. Generally, curved linear excision provides patients with any degree of cosmetic appearance they desire but does not maintain the appearance of the dark and irregular edges. The more radical reductions are not possible with wedge techniques. • Most women undergoing minoraplasty want the dark edges of the labia minora removed, but some prefer to preserve the dark natural-looking edge and request only reduction of the labial bulk.2,3 More aggressive resections and exacting excisions are possible with curved linear resections as opposed to wedge techniques. • Emerging evidence supports the increased safety, precision, functional, and aesthetics of radiofrequency (RF) labia minora labiaplasty, compared with other minora reduction procedures, performed by a properly trained and experienced practitioner.4 Labiaplasty, which is sometimes called labioplasty, is a gynecologic surgical procedure to reduce the size and sometimes the shape of either the labia majora or labia minora.5,6 It is currently one of the most frequently performed aesthetic vaginal surgical procedures.5 The bilateral longitudinal mucocutaneous folds between the labia majora and vulvar vestibule are called nymphae or labia minora.6–8 The labia minora are extremely sensitive to touch during sexual stimulation because of the erectile connective tissue and rich nerve endings in the nymphae.5 The minora vary widely in length, thickness, symmetry, protuberance, and the degree to which they project beyond the edge of the labia majora.5,6,8,9 Rarely, the minora protrude more than 3 cm beyond the free edge of the labia majora5–10 and are often considered hypertrophic and aesthetically displeasing. The cause of hypertrophic labia minora can be multifactorial and includes congenital 8,11 and acquired idiopathic hypertrophy12,13 from intercourse or possibly masturbation, childbirth by the vaginal route, lymphatic stasis, inflammation from dermatitis or urinary incontinence,5 and stretching with weights and exogenous androgenic hormones.13 In 1984 Hodgkinson and Hait14 described their experiences with labiaplasty on three women unhappy with the size and bulkiness of their labia minora. Their study led to the first published report on elective cosmetic reduction surgery of the labia minora designed for visual improvement of the external genitalia in Western women. The main surgical techniques currently used in labia minora reduction include curved linear excision (sometimes referred to as cutting or amputation techniques) or elliptical excision3,8,14 (also called longitudinal resection or trimming of the labial edges with oversewing of the labial edge),3,15,16 central wedge resection,17 modified V-wedge resection (V plasty),18,19 deepithelialization,13,20 laser labiaplasty,21 and RF labiaplasty. Regardless of the technique employed, labia minoraplasty procedures should not damage the neurovascular supply or the introitus. A viable labiaplasty should preserve the contour of the lips, when requested by the patient, and the color and texture of the labial edge, or the labia minora should be removed, if requested.3,8 Patients are given an in-office, local anesthetic (0.25% Marcaine or 1% lidocaine with 1:100,000 epinephrine), conscious sedation, or traditional general anesthesia.3,5 In 2005 I reported on a minimally invasive surgical procedure popularly called the Barbie look (Fig. 5-1).3 This is a slang term used by patients in Los Angeles who requested removal of all or almost all of the labia minora. The rim look and the hybrid look procedures were also described (Figs. 5-2 and 5-3). The rim look procedure involves a curved linear vertical excision of only the dark edges of the labia minora to smoothen and even them. They should protrude past the labia majora. The hybrid look refers to a finessed, middle-road approach involving removal of nearly all of the labia minora and preservation of a petite “peekaboo” (below or to the level of the labia majora) amount of tissue that appears more attractive to some patients.3 This degree of precise excision of labial tissue is possible with the use of RF pinpoint “hair” tips. This exact degree of tissue removal cannot be satisfactorily achieved with wedge techniques. Fig. 5-1 This patient is shown before and after having a Barbie look procedure. Fig. 5-2 This patient is shown before and after having a rim labiaplasty. Fig. 5-3 This patient is shown before and after having a hybrid labiaplasty. Regional preferences for the Barbie look vary significantly, with a greater preference reported on the West Coast than on the East Coast or in the South. In a study of 238 women considering labial reduction, 98% sought a labia minora reduction to the level of or below the level of the labia majora.22 In my survey4 of 200 patients, none preferred to retain the contour and/or darkness of the corrugated free edge. Instead, all patients requested removal rather than retention of the dark edges. In my experience, it is extremely rare for a woman to ask her surgeon to leave the dark labial edges intact during a labiaplasty. In Miklos and Moore’s study22 of 550 women, 97% wanted removal of the dark edges (preferring pink edges), which resulted in a smoother contour of the labial free edge. Wedge techniques are ideal for females seeking to retain the dark edges or the natural contours of the labia minora. A wedge resection, a full-thickness excision, and modifications of this technique are sometimes preferable for minimizing nerve injury, scarring, and overresection that can lead to an excessively tightened introitus.8,11 In 1998 Alter11 introduced modifications of the wedge resection, including a central wedge resection with an external wedge (hockey stick V),8,17 a 90-degree Z-plasty,5,7 an inferior wedge resection,23 and Maas and Hage’s zigzag technique.8,24 An extended central wedge resection incorporates an external wedge (hockey stick V) to remove excess lateral clitoral hooding or dog-ears.8,17 This approach is associated with less wound edge separation, sinus/fistula formation, clitoral hood excess, and postoperative pain, although absolute numbers of affected patients are limited and the number of patients with these complications is not always reported.8 The addition of a 90-degree Z-plasty to the central wedge excision spreads the tension over the suture line, thus minimizing traction on the suture line.5,7 In an inferior wedge resection approach, the wedge is removed in the inferior part of the labia, and the superior pedicle is used to reconstruct the labia.23 Maas and Hage’s zigzag technique8,24 is another modification of a wedge excision. It involves a W-shaped resection with interdigitated suturing of the protuberant labium. The downsides of wedge-type labiaplasty surgery are the variable blood supply of the labia and the tension on the outward pulling edges. Wedge-type labiaplasty carries increased risk for improper healing, holes in the labia, and distinct pizza-shaped gaps when the edges pull apart.3 These complications have not been reported in curved linear resections performed by qualified surgeons. Surgical techniques may be combined, if warranted, with different methods sometimes used on each labium.8 In bilateral deepithelialization both the medial and lateral sides of each small vaginal lip are marked to delineate excisable areas, and both sides are deepithelialized, or “skinned off,” with either a scalpel or laser. The procedure is performed in approximately 30 minutes. The technique is advantageous if only a minimal amount of labia tissue needs to be excised.25 However, if a large area must be deepithelialized, the approach may result in a redundant free border, increased labial thickness with bunching, wound necrosis and breakdown, and an abrupt color change at the suture line.5,25 Laser labiaplasty has not been shown to be advantageous in repairing the labial edge after the excess tissue is trimmed. Although laser labiaplasty is used in the deepithelialization technique, it increases the risk for development of epidermal inclusion cysts.5 Furthermore, deepithelialization can interfere with the labial blood supply, resulting in holes and gaps in healing.4 In the past decade the use of RF-based excision and revision surgery in aesthetic vulvovaginal surgery has increased. RF labiaplasty was first performed and reported in 2005 and presented in 20063 at the meeting for the American Academy of Cosmetic Gynecologists. This technique is especially suitable for labiaplasty surgery, because the minimal lateral thermal spread is only 20 to 40 µm when the procedure is performed with a hair-tip attachment. No discernable edge burn or scarring is visible, and no bubbling of skin occurs. Both of these features lead to improved safety during delicate surgery around the clitoral region. RF technology also allows feathering of irregular edges and smoothening and flattening of the dog-ears. RF incisional and excisional surgery can be performed with all techniques described. It is most frequently used with curved linear excisions. This technique is described at length here. Labia minora reduction surgery may be performed for functional or aesthetic reasons or both. Functional indications of labia minoraplasty include difficulty maintaining hygiene (for example, because toilet paper sticks), chronic chafing of the pudendal skin, irritation when wearing tight clothing, pain during bicycle riding and similar sports activities, and the labia catching in zippers.5,9,15,18,25 Many women undergo labiaplasty for aesthetic reasons, particularly because of the appearance of a bulge under their clothing 3,5,19,25 or because of enlarged inner vaginal lips that cause embarrassment during sexual relations.18,26 Because the causes for undergoing this procedure typically involve both cosmetic and functional issues, labia minoraplasty is equally a medical therapeutic intervention and a cosmetic surgical procedure. There are no absolute contraindications to labiaplasty; relative contraindications include active gynecologic infections and malignancy.5 Patient consultations are preferably carried out days before surgery but may occur on the same day as surgery, with special arrangements such as a prior Internet consultation. For example, an athletic runner may present in the office with complaints of uneven labia that are embarrassing and painful. Her prior rectocele repair was successful but resulted in asymmetrical labia, with a constant pulling sensation. She requests a labiaplasty to remove almost all the labia minora on both sides, preserving a small amount of labia for a more natural look. The patient is given a mirror to ensure that she and the surgeon are discussing the same structures. On physical examination, the left labia are twice the size of the right labia and are thicker with darker edges. She may request a more symmetrical appearance and removal of the darkened edges. The clitoral hood is not bothersome to the patient, but she does not want a “top heavy” look after labial reduction. A clitoral hood reduction is recommended for some patients to provide a more symmetrical appearance. Preoperative photographs are taken with the patient in various positions. Examining the patient when she is lying down and standing can help to show the anatomy involved and to confirm the requested amount of labial tissue to remove and the desired, ideal appearance. They are reviewed with the patient so that she can envision the appearance of her labia once they are healed and to help her decide the amount of labia to remove and whether a clitoral hood reduction would be aesthetically beneficial. After extensive discussions with the patient, a decision is made and documented with drawings and/or photographs. The patient is screened for her general health, allergies, pregnancy status, anxiety, tolerance to pain, understanding of the procedure, and a detailed consent is obtained. Approximately 2 hours before surgery, the patient places numbing cream (EMLA or compounded topical anesthetics) on the surgical sites. When labiaplasty is carried out in the office, dermoelectroporation is performed for 15 to 30 minutes to push the macro-molecular numbing cream under the skin to provide comfort during the placement of local anesthesia (Fig. 5-4). Oral or intramuscular narcotics are given in combination with an anxiolytic agent such as Valium.
Labia Minora Reduction Surgery: Curved Linear Resection
Red Alinsod
Key Points

Alinsod Surgical Technique for Radiofrequency Labia Minoraplasty
Indications and Contraindications
Patient Evaluation
Preoperative Planning and Preparation
Anesthesia

Related posts:
 Fractional Erbium Laser for Vaginal Rejuvenation
Fractional Erbium Laser for Vaginal Rejuvenation
 Labia Majora Reduction Surgery: Majoraplasty
Labia Majora Reduction Surgery: Majoraplasty
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
 Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
 Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine
