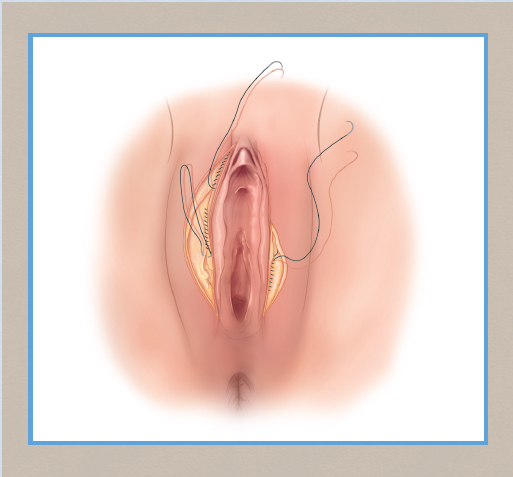
CHAPTER 6 • Labia majoraplasty is generally well tolerated and associated with favorable clinical outcomes. • Removal of excess, loose skin does not appear to damage large vessels or nerves or affect sensitivity of the skin. • Bleeding is an important potential complication when fat pad excision techniques are employed and larger deeper vessels are transected. • Pain control is more challenging after fat pad removal. • Preliminary findings suggest that high-frequency monopolar radiofrequency (RF) and standard electrocautery are beneficial surgical tools in labia majora reduction surgery. • Labia minoraplasties and labia majoraplasties may be performed as staged operations in the same patient. When performed by surgeons with advanced training, a combined and unified approach to simultaneous labia minoraplasty and labia majoraplasty is practical and safe in selected patients. The labia majora, composed largely of fatty tissue, are bilateral structures of the vulva that extend from the bottom of the mons pubis to the rectum.1,2 Anatomic variation in the length and volume of the labia majora is normal and does not usually indicate a pathologic condition. The length is 7.0 to 12.0 cm, with a mean measurement of 9.3 cm.3 Hereditary and environmental factors may contribute to individual variance in the size and shape of the labia majora. With a loss of volume, the labia majora may droop or sag with aging and after bariatric surgery4,5 (Fig. 6-1). Excess fat deposits (genetic or from general obesity) can enlarge and stretch the labia majora. Prominent skin laxity of the labia majora in patients who have had significant weight loss can be quite astounding and distressing and may require RF shrinkage or surgical reduction.6 Prominent or bulky labia majora may be problematic for some women, typically by causing an embarrassing bulging under pants, swimsuits, and tight-fitting clothing.6–8 They may lead to functional problems with sexual intercourse, poor hygiene, and physical discomfort in the genital region. Examples of those affected include bikers, horseback riders, and rowers who have chronic vulvar rubbing.9,10 Some women have lowered self-esteem because of the undesirable physical appearance of their majora.6 A common derogatory, slang term for hypertrophic and visually unappealing labia majora is camel toes.9,10 Several websites unfairly highlight “camel toes” in young celebrities, which actually are normal and healthy labia majora. However, some women are born with very prominent fat pads in the labia majora. Symptomatic labia majora issues that warrant medical attention are typically seen in middle-aged to older women but rarely in, for example, 21-year-old women.10 Fig. 6-1 The aging vulva and vagina. Bikini shaving, effects of gravity, and decreased collagen, elastin, and volume are contributing factors in the rise of labia majoraplasty surgery. Labiaplasty is a plastic surgical procedure performed to reduce the size of hypertrophic labia, usually to improve the aesthetic appearance of the vulval area.1,5,7,10–12 It involves removal of excess labia majora skin and prominent fat pads and is akin to a modified radical vulvectomy but without excision of groin lymph nodes. Rarely, this technique is employed to dramatically reduce the uncomfortable edema from congenital lymphedema of the vulva.9 Labial reductions are typically performed on the labia minora and increasingly on the labia majora of female baby boomers, in whom aging often leads to sagging majora.9 Primary labia majora hypertrophy results from volume excess from fat deposits, whereas secondary labia majora excess is caused by volume loss, leading to skin excess.5,7 Labia majoraplasty is performed for either aesthetic or functional purposes or both and less commonly than labia minoraplasty. Reduction of the majora tissue is indicated for patients with hypertrophic labia majora over a wide range of ages, and for those who have undergone substantial weight and fat loss with resultant majora laxity.7,10 In affluent communities, such as the beach cities in the United States, the demand for labia majoraplasty is on par with the demand for labia minora reduction.9,10 Contraindications include undiagnosed vulvar lesions and vulvar dystrophies, active infectious lesions such as herpes and human papillomavirus. Relative contraindications include foreseen large-weight loss that may result in more skin laxity of the majora. Weight loss should preclude surgical labia majoraplasty. The patient is evaluated while she is in a lithotomy position and also while she is standing to best assess the anatomy involved and to confirm her desired, ideal appearance. The extent of the labia majora laxity is evaluated and photographed to help plan the surgical course of action. Markings may be placed to show looseness and asymmetry and the location of the suture lines. During the examination, the patient is given a mirror for visualizing the area to ensure she and the surgeon are discussing the same structures. The patient can point out the areas of concern and show how much tissue needs to be removed. By manually manipulating the labia majora, the surgeon can approximate the patient’s desired postoperative appearance. The surgeon can explain that overly aggressive removal of labia majora tissue can result in pulling open of the lateral vaginal opening, creating a gaping vagina. Carefully asking whether this will be bothersome is essential. A more aggressive reduction can be performed in patients who do not mind a pulled-open appearance of the vaginal opening. However, less tissue removal is best for those concerned about the aesthetic appearance of the vaginal opening. Surgeons should stress that moderation is the goal for surgery. A general physical examination and a pregnancy test in women in their reproductive years are recommended. Other blood work, such as a CBC and electrolytes, is typically not necessary in healthy women. Other specific tests can be ordered on a case-by-case basis. After extensive discussions, the surgeon and patient agree on a plan, which is documented with drawings and/or photographs of how much tissue will be excised. Detailed consent is obtained once the patient has been screened and has clearly stated her desired amount of reduction of labia majora tissue. Patients are instructed to place a numbing cream (EMLA or compounded topical anesthetics) on the surgical sites approximately 2 hours before surgery. When labia majoraplasty is performed in the office, dermoelectroporation can be performed for 15 to 30 minutes to push the macromolecular numbing cream under the skin to provide comfort during the placement of local anesthesia. Approximately 10 ml of a local anesthetic with epinephrine should be prepared with the use of a 30-gauge needle to prevent overdistension of tissue. Oral or intramuscular narcotics are given in combination with an anxiolytic agent such as Valium or Ativan. A long-acting liposome-coated local anesthetic, such as Exparel, is ideal as an adjunct for postoperative pain control; this can last 72 hours or more. If Exparel is used, lidocaine must not be included, because it appears to break down the liposome and reduces the duration of effect of Exparel. Fig. 6-2 shows typical markings. A vertical line is marked, beginning at the top level of the clitoral hood and extending in the labial crease, between the lateral labia majora and the medial clitoral hood and labia minora. The line is drawn down to the level of the introitus. A semielliptical mark is made from the top of the vertical line and extending laterally just past the top ridge of the labia majora, curving back down toward the lowest point of the vertical line. This is repeated on the opposite side for symmetry. Excising a moderate amount of labia majora tissue is recommended to prevent the appearance of a gaping vaginal opening, which occurs if excess labia majora is removed, as discussed previously. The patient is placed in a low lithotomy position with adequate support of the legs to ensure comfort and good blood flow. Support under the knees and calf is recommended over simple heel support. Fig. 6-2 Markings on the crease between the labia minora and labia majora are made with a standard medical skin marker. Hugging the curves and lines of the clitoral hood region and labia minora medially will help to better hide suture lines. Excess skin removal is advised.
Labia Majora Reduction Surgery: Majoraplasty
Red Alinsod
Key Points

Indications and Contraindications
Patient Evaluation
Preoperative Planning and Preparation
Surgical Technique
Anesthesia
Markings
Patient Positioning

Related posts:
 Fractional Erbium Laser for Vaginal Rejuvenation
Fractional Erbium Laser for Vaginal Rejuvenation
 Labia Majora Reduction Surgery: Majoraplasty
Labia Majora Reduction Surgery: Majoraplasty
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
 Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
 Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


