, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
With special contributions from Haider Mejbel, MD, Baylor College of Medicine.
23.1 Apocrine Cystadenoma
23.1.1 Clinical Features
23.1.2 Histology
Histologic sections demonstrate skin with a cystic proliferation within the dermis. Two types of cells are seen in the cyst lining. Eosinophilic cuboidal cells with decapitation secretion are seen emptying into the lumen. Another layer of myoepithelial cells is present in most cases [3]. This lining demonstrates papillary infoldings into the luminal cavity with true fibrous papillary cores within the papillae. Mitotic activity is present, but cytologic atypia is not seen [2, 4]. Mucinous metaplasia of closely apposed eccrine ducts has been reported. The relationship between the eccrine structures and this neoplasm is not apparent [1].
23.2 Eccrine/Apocrine Hidrocystoma
23.2.1 Clinical Features
Multiple hidrocystomas most often occur in middle-aged to elderly females, while solitary lesions are seen with equal frequency in males and females [5]. Although uncommon, hidrocystoma has been reported in children. Hidrocystomas are characterized by shiny, skin-colored to slightly bluish cystic nodules and smaller papulonodules on the face [5, 6]. Apocrine hidrocystomas typically are solitary, occurring along the eyelid, while eccrine hidrocystomas are more commonly multifocal and may enlarge with heat exposure [5, 6]. Hidrocystomas are benign with no known reports of malignant transformation.
23.2.2 Histology
Biopsy of hidrocystoma demonstrates a dermal cystic cavity lined by two thin layers of cuboidal epithelium that resemble eccrine ductular epithelium (Fig. 23.1). Features of apocrine glandular epithelium are not present. Eosinophilic eccrine secretions are found in a minority of cases. In some cases, the cyst is lined by cells with apocrine differentiation (Figs. 23.2 and 23.3).
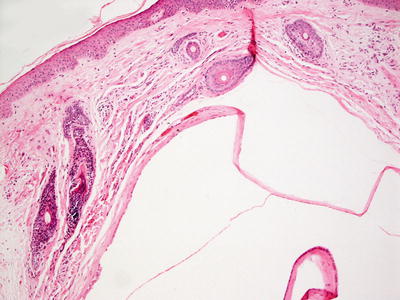
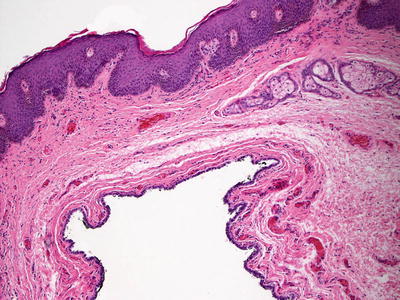
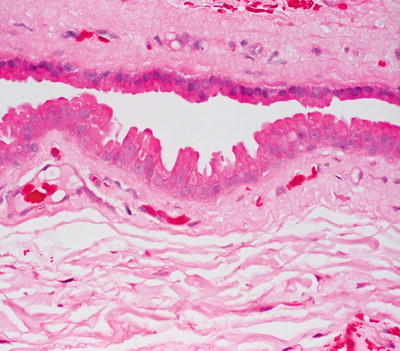
Fig. 23.1
Eccrine hidrocystoma demonstrates a thin-walled cystic structure lined by a flattened epithelium
Fig. 23.2
Apocrine hidrocystoma is a cystic structure in the superficial reticular dermis that is lined by apocrine-type epithelium
Fig. 23.3
Hobnailing of the luminal epithelium with brightly eosinophilic cytoplasm is seen in apocrine hidrocystoma
23.2.3 Pathogenesis
Eccrine hidrocystoma is a cyst of eccrine sweat ducts. A possible factor in hidrocystoma formation is duct obstruction due to increased sweat production [7]. Interestingly, botulinum toxin A, which denervates the sweat glands and reduces sweating, has been used effectively in the treatment of eccrine hidrocystoma [8], thus implicating a role for enervation and sweat production in its formation.
23.3 Branchial Cleft Cyst
23.3.1 Clinical Features
Branchial cleft cysts are an uncommon anomaly of the branchial apparatus, most frequently the second arch [9]. They usually present in the second or third decade of life. Branchial cleft cysts are soft, skin-colored nodules along the lateral aspect of the neck at the anterior border of the sternocleidomastoid muscle. Lesions slowly increase in size over time, and may become red and tender following infection or rupture [9]. As the cysts are at risk for infection, surgical excision is recommended once lesions are found.
23.3.2 Histology
Branchial cleft cysts arise from one of four branchial clefts, and demonstrate variable histologic changes depending upon the site from which they arise [10, 11]. The epithelial cyst lining may be either squamous or columnar with ciliated respiratory epithelium (Fig. 23.4). Some cases demonstrate both types of lining [10]. Cutaneous appendages may be present in some cases [11]. The constant feature is a dense lymphoid infiltrate that extends into the lining epithelium regardless of cell type. Prominent germinal centers can be observed. Mucous glands and cartilage are variably present. Older lesions may have fibrosis and granulation tissue consistent with prior rupture and inflammation .
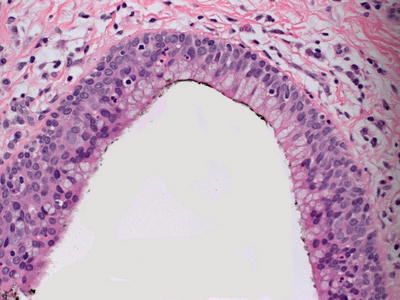
Fig. 23.4
Respiratory-type columnar and ciliated epithelium lines a cystic space and is surrounded by lymphocytes in a branchial cleft cyst
23.3.3 Pathogenesis
The origin of branchial cyst is not known. Some authors have proposed that the origin of a branchial cleft could depend on the anatomic location. Cysts in the upper neck region could develop from salivary gland inclusions in parotid lymph nodes, or from epithelial remnants of the upper portion of the branchial apparatus [12]. Cysts in the mid-neck region could develop from epithelial remnants of the cervical sinus or the branchial pharyngeal pouches. Cysts in the lower neck area could develop from remnants of the thymic duct or from the lower portions of the branchial apparatus .
23.4 Bronchogenic Cyst
23.4.1 Clinical Features
The exact incidence of bronchogenic cyst is not known. Boys appear to be more commonly affected than girls. There is no reported racial predilection [13, 14]. Bronchogenic cyst presents as a solitary subcutaneous nodule, and it can have associated fistula or verrucous change. Lesions are commonly located at the presternal notch, followed by the neck and scapula. Limited data exists on long-term prognosis as many of the cysts are excised in childhood. Recurrence may occur with incomplete excision.
23.4.2 Histology
Histologic findings of bronchogenic cyst include a cystic structure lined by cuboidal or columnar epithelium that may be pseudostratified and ciliated [15] (Figs. 23.5, 23.6 and 23.7). Surrounding the epithelium are concentric smooth muscle bundles and fibrous tissue. Cartilage may be present in some cases, and mucous glands are sometimes encountered [16]. In rare cases, the presentation may be that of a polypoid lesion or a nodule [17, 18]. Branchial cleft cysts demonstrate a brisk lymphoid infiltrate within the cyst wall, which is a distinguishing feature not seen in bronchogenic cysts.
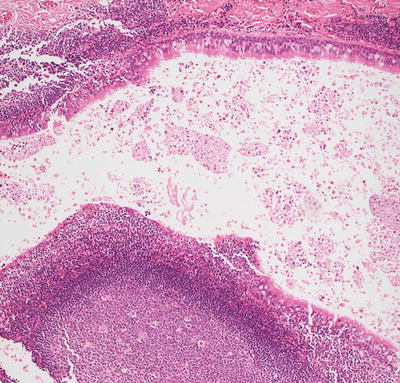
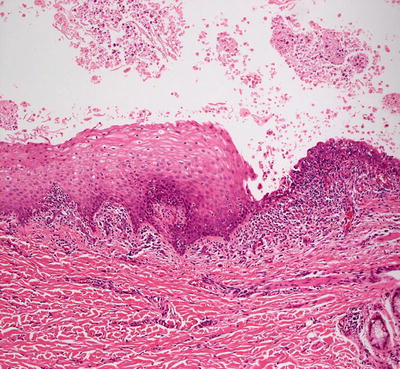
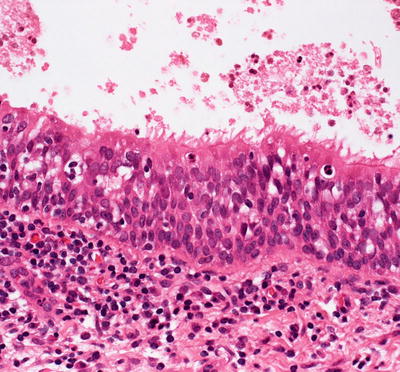
Fig. 23.5
Respiratory-type columnar epithelium lines a cystic cavity in bronchogenic cyst
Fig. 23.6
In some bronchogenic cysts , both columnar and squamous epithelium can be seen in the lining epithelium
Fig. 23.7
Ciliated epithelium lines some bronchogenic cysts
23.4.3 Pathogenesis
Bronchogenic cyst is a type of bronchopulmonary malformation. It has been proposed that the cyst results from a developmental error in the budding of the foregut [19, 20]. The primitive foregut is the origin of the respiratory tract and esophagus. Abnormal budding of the tracheal primordial may lead to the formation of the cyst. Bronchogenic cyst in children has been found in unusual anatomic locations, such as the scapula, and has been attributed to heterotopia and metaplasia of the growth of respiratory epithelium in the skin [21].
23.5 Thyroglossal Duct Cyst
23.5.1 Clinical Features
Thyroglossal duct cysts are the most common congenital cyst of the neck [9]. They may be located anywhere along the tract between the posterior tongue and the superficial anterior neck. The cyst presents as a slowly expanding, mobile midline nodule that moves with swallowing secondary to its attachment to the hyoid bone.
Patients with thyroglossal duct cysts may be at risk for development of papillary thyroid carcinoma in adulthood, although this is rare [9]. Cysts are also at risk for infection and rupture with subsequent inflammation. Because of this potential for complications, surgical excision is encouraged.
23.5.2 Histology
Biopsy of thyroglossal duct cyst demonstrates a fibrous tract lined by stratified squamous or pseudostratified ciliated columnar or cuboidal epithelium, depending upon the anatomic relationship with the hyoid bone [22] (Fig. 23.8). Within the cyst wall, ectopic thyroid tissue can be identified (Fig. 23.9). In some cases, this tissue may function and lead to clinical symptoms. Most cases display a dense lymphoid infiltrate, and mucus glands may be present in some cases. Fine needle aspiration biopsy yields an accurate diagnosis in most cases, demonstrating thyroidal colloid, macrophages, and neutrophils [23]. It is unusual to identify the lining epithelium with this technique, and most authors do not recommend fine needle aspiration for establishing a diagnosis [23, 24]. Rare malignant transformation has been reported in thyroid tissue [25, 26].
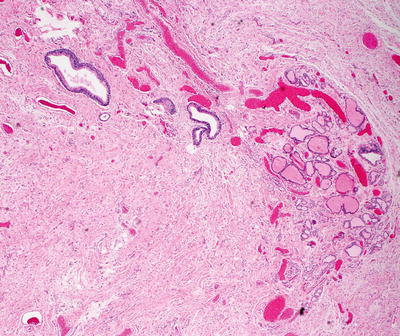
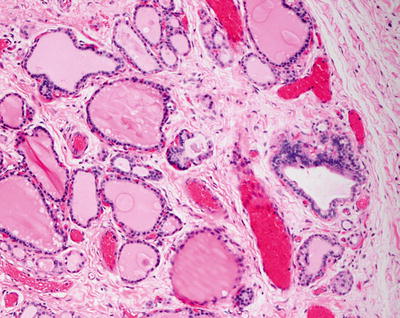
Fig. 23.8
Thyroid ducts and glands are present within the dermis in a thyroglossal duct cyst
Fig. 23.9
Thyroid glands with colloid material are seen within the well-formed glandular structures in a thyroglossal duct cyst
23.5.3 Pathogenesis
During embryogenesis, the median thyroid anlage elongates proximal to the descending gland, forming the thyroglossal duct. This duct generally obliterates by week 5 of gestation. However, failure of the thyroglossal duct to obliterate before the formation of the mesodermal anlage of the hyoid bone results in its persistence during development [27]. Other studies suggest that proliferation of remnants of the thyroid gland and the thyroglossal tract may be stimulated by inflammatory processes, and inflammatory reaction to infection during childhood may stimulate epithelial remnants of the thyroglossal tract to undergo cystic changes [28].
23.6 Dermoid Cyst
23.6.1 Clinical Features
Dermoid cysts are congenital anomalies occurring over embryonic fusion lines. They may slowly expand over time, leading to delayed appearance and subsequent diagnosis [29]. Dermoid cysts present as non-translucent, mobile subcutaneous, blue or skin-colored nodules. They are frequently seen on the orbital ridge along the lateral eyebrow. Approximately 3 % of lesions are located at the nasal midline, with an increased risk for deep extension and central nervous system (CNS) involvement [9]. Associated dimple, ostia, or hair tuft increases the likelihood of intracranial extension or associated CNS malformation.
23.6.2 Histology
Being true epidermal inclusions cysts, dermoid cysts contain all epidermal components. Within the mid-reticular dermis, a cystic cavity that is often filled with keratin is apparent. The cyst wall is lined by stratified squamous epithelium, complete with a granular layer. Pilosebaceous units emanate from the cyst lining into the surrounding dermis (Figs. 23.10 and 23.11). Apocrine and eccrine ducts are present, and smooth muscle bundles are seen in a minority of cases. In some dermoid cysts occurring close to the eyes, conjunctival type mucosa with goblet cells have been reported in the cyst lining [30]. When the cysts have been traumatized, a granulomatous foreign body giant cell reaction may ensue [31]. Late lesions may flatten and only dense fibrosis is apparent in senescent lesions [32].
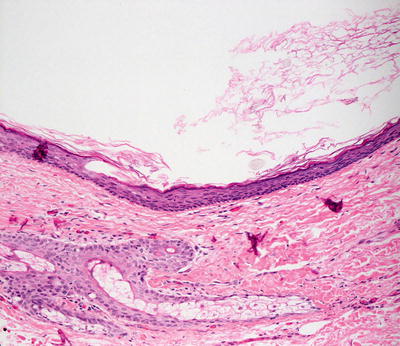
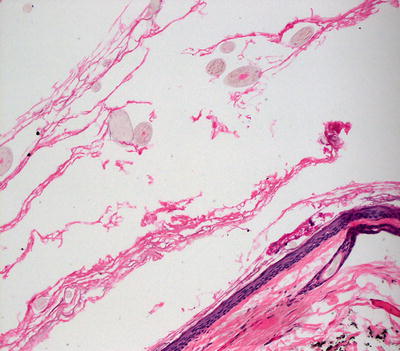
Fig. 23.10
A dermoid cyst demonstrates squamous epithelium, keratinaceous cyst contents, and cutaneous appendages in the wall of the cyst
Fig. 23.11
Vellus hairs, squamous epithelial lining, and cutaneous appendages in the cyst wall are seen in dermoid cysts
The differential diagnosis may include a follicular cyst of the infundibular type, also called epidermal inclusion cyst. Since this name is a misnomer, cutaneous appendages are not present within the cyst lining in these cysts. The cyst lining cells are derived from dilatation of follicular units at the level of the follicular infundibulum .
23.6.3 Pathogenesis
Cutaneous dermoid cyst is a type of congenital cyst that is derived from the ectoderm and mesoderm. It is formed from epithelial rests found along embryonic fusion lines and contains cutaneous structures such as keratinizing squamous epithelium and hair follicles [33].
23.7 Follicular Cyst
23.7.1 Clinical Features
Follicular cysts most commonly occur in young and middle-aged adults, and rarely occur in childhood [34]. Multiple lesions may be seen as a clinical feature of Gardner syndrome, especially with generalized distribution at the face, scalp, trunk, and extremities. Follicular cysts are characterized as 1–2 cm subcutaneous dome-shaped nodules with an overlying punctum. The overlying skin may be red and tender when inflamed.
Vellus hair cysts are more common in children. Eruptive vellus hair cysts appear as multiple small folliculocentric cysts on the trunk (Fig. 23.12). Solitary lesions are amenable to excision. When cysts are inflamed, incision and drainage or treatment with oral antibiotics may be required.

Fig. 23.12
Eruptive vellus hair cysts present as multiple brown, hyperpigmented 1–2 mm folliculocentric papules on the central trunk
Pilar cysts are far less common than follicular cysts. They occur most frequently in middle-aged women [34]. Pilar cysts typically present as skin-colored, slightly mobile, smooth and firm subcutaneous nodules without an overlying punctum. The great majority of pilar cysts occur at the scalp [34]. Solitary lesions exist but they are frequently multiple. If desired, lesions can be removed surgically often without rupture .
23.7.2 Histology
There are several types of follicular cysts that arise from different portions of the hair follicle. The most common, frequently misnamed as an epidermal inclusion cyst or a sebaceous cyst, arises from the infundibular portion of the hair follicle (Fig. 23.13). Keratinizing epithelium that has a granular layer with prominent keratohyalin granules forms the cyst lining. The cyst wall typically lacks rete ridge formation, and dermal appendages do not emanate from it. The lack of appendages distinguishes this from a dermoid cyst, which is truly an invagination or inclusion cyst of the epidermis. The cystic cavity is filled with wispy keratin that resembles normal stratum corneum .
Fig. 23.13
A follicular cyst is filled with wispy orthokeratotic keratin and lined by epidermis that has a granular layer
Another type of follicular cyst is a pilar or isthmus-catagen cyst. These cystic dilatations arise from the isthmus portion of the hair follicle and, as such, are lined by stratified squamous epithelium that lacks a granular layer. There is abrupt keratinization, and the cyst cavity is filled with densely packed and hyper-eosinophilic keratin (Fig. 23.14). The cyst epithelium can proliferate, resulting in heaping up of the epidermis. Mitotic activity is readily apparent in these situations, and there can be some cytologic atypia. Proliferating pilar tumors may give rise to the differential diagnosis of squamous cell carcinoma, although they do not grow down from the surface epithelium. In addition, they are well circumscribed and not invasive. Squamous cell carcinoma would be most uncommon in this setting in the pediatric age group.

Fig. 23.14
A pilar cyst is lined by squamous epithelium that lacks a granular layer and is filled with dense, compact orthokeratotic keratin
Vellus hair cysts are simple cysts lined by stratified squamous epithelium with a granular layer. The cystic space is filled with wispy stratum corneum-like keratin, and many small vellus hairs are present (Fig. 23.15).
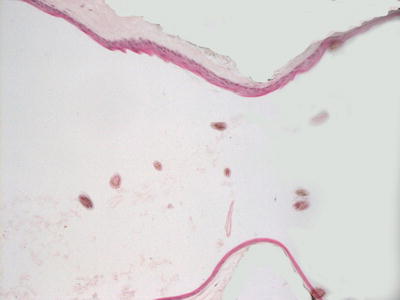
Fig. 23.15
A vellus hair cyst is lined by squamous epithelium and contains wispy keratin and abundant vellus hairs
23.8 Human Papillomavirus-Related Cyst
23.8.1 Clinical Features
The incidence of human papillomavirus (HPV)-related cysts is unknown, and reports in the literature are few, suggesting that this is a rare phenomenon. Lesions are primarily described in adults, although there are cases in older adolescents [38]. Lesions frequently are reported to follow trauma. There is no reported gender or racial predilection. HPV-related cysts, located on acral sites, are skin-colored subcutaneous cystic nodules without overlying verrucous change that mimic the appearance of an epidermoid cyst [39].
23.8.2 Histology
Biopsy changes include cystic structures occurring primarily on acral skin. The cystic lining consists of keratinocytes with foci of hypergranulosis and overlying parakeratosis within the cystic cavities. Papillomatous processes extend into the luminal cavity, and vacuolated keratinocytes are present at the tips of the projections. Keratinocytes in the cells demonstrate marked hyperkeratosis [40]. Amorphous eosinophilic cytoplasmic inclusions appear within keratinocytes in the uppermost layers of the cyst lining cells [41]. The so-called ridged warts demonstrate similar histologic changes, although without the cyst formation and similar cytoplasmic viral inclusions [39].
23.8.3 Pathogenesis
HPV-related cysts have been postulated to develop from eccrine ducts and are commonly associated with HPV-60 and sometimes HPV-57 subtypes [43–45]. It has been proposed that HPV initially infects the upper part of the eccrine duct and then migrates into the dermal portions of the eccrine duct, where virus-associated cysts develop [39]. Other studies have suggested that a combination of ultraviolet light exposure and HPV infection is a risk factor for the formation of cysts [39, 46].
23.9 Median Raphe Cyst
23.9.1 Clinical Features
Patients with median raphe cyst typically present in the second or third decade of life, although pediatric cases exist [47]. Median raphe cyst can occur anywhere between the urinary meatus and the anus. It most commonly presents as an asymptomatic, skin-colored to bluish subcutaneous nodule along the ventral aspect of the penis, near the glans penis [47]. Following persistent friction or trauma, the lesion may become inflamed with secondary infection. Surgical excision is the treatment of choice and is curative.
23.9.2 Histology
Histologic findings of median raphe cyst are those of a cystic structure within the mid-reticular dermis lined by pseudostratified columnar epithelium (Figs. 23.16 and 23.17) [47–49]. Some of the lining cells may be ciliated, columnar, or squamatized [50–52]. Mucinous cells are present in a minority of cases [48]. Rare cases are described in which abundant melanocytes are present within the cyst lining, giving the cyst a pigmented appearance [53, 54].
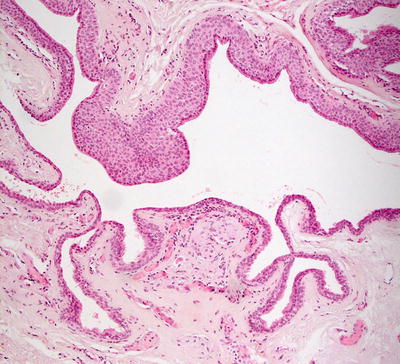
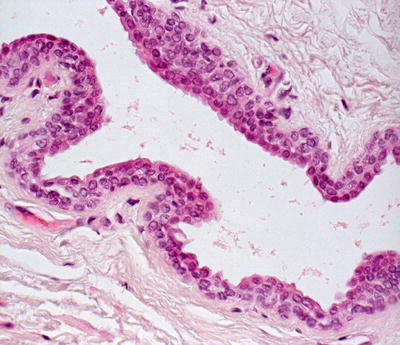
Fig. 23.16
There are two or more layers of cells lining a cystic cavity in a median raphe cyst
Fig. 23.17
The luminal cells demonstrate a hobnail pattern of growth into the lumen in a median raphe cyst
23.9.3 Pathogenesis
Median raphe cyst is thought to be an embryologic developmental defect of the male genitalia. It has been proposed that the cyst represents embryologic split-off outgrowths of the epithelium after primary closure of the urethral or genital folds. Others suggest that median raphe cyst arises from epithelial rests incidental to incomplete closure of the folds [55, 56].
23.10 Cutaneous Ciliated Cyst
23.10.1 Clinical Features
23.10.2 Histology
While cutaneous ciliated cysts are much more predominant in young girls, they have also been described in boys and men, and are thought to be of Mullerian origin [58, 59]. Histologic findings demonstrate a dermal-based cyst lined by ciliated cuboidal or columnar cells (Fig. 23.18). Squamous metaplasia, apocrine change, and cells producing mucin have been described in these lesions, but they are not common findings [60, 61].
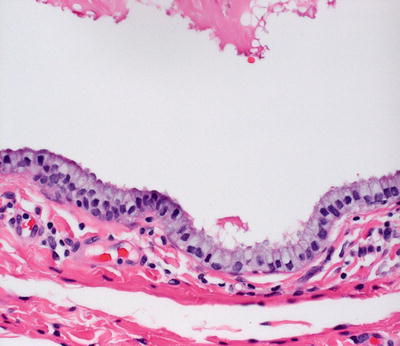
Fig. 23.18
A cutaneous ciliated cyst is lined by columnar epithelium with delicate cilia extending into the cystic cavity
Positive immunohistochemical staining with antibodies against PAX-8, progesterone receptors and epithelial membrane antigen as well as lack of staining for carcinoembryonic antigen suggests that despite the anatomic proximity to eccrine structures in some cases, these cyst are not derived from eccrine ducts or glands [57, 62–64].
23.10.3 Pathogenesis
It has been proposed that cutaneous ciliated cyst in females is a result of heterotopia and sequestration of Mullerian tissue [65]. Supporting evidence for this theory includes the predilection of cyst for the lower extremities, and its resemblance to fallopian tube tissue histologically. Cutaneous ciliated cyst also expresses molecular markers similar to the fallopian tube in terms of estrogen, progesterone, and PAX-8 expression [66–68].
23.11 Steatocystoma
23.11.1 Clinical Features
Steatocystomas commonly occur in adolescence, during and following puberty. Solitary lesions present at birth and in early infancy have been reported as well [69]. Steatocystoma multiplex is a rare autosomal dominant disorder with high penetrance, and is characterized by multiple steatocystomas [69, 70].
Steatocystomas present as 0.5–2 cm, skin-colored to yellowish subcutaneous cystic nodules, primarily localized to the chest, although they may sometimes appear on the face, genitals, arms and thighs (Fig. 23.19) [70]. Widespread involvement may occur with palmoplantar sparing. Lesions express an oily material when punctured. Patients may also have eruptive vellus hair cysts, most notably in the setting of pachyonychia congenita. Lesions are rarely symptomatic, but may be surgically excised or incised and drained.

Fig. 23.19
Steatocystoma presents as a subcutaneous nodule without overlying skin changes at the axilla in an adolescent girl
23.11.2 Histology
Histologic changes of steatocystomas are identical regardless of whether the lesions are single (simplex) or multiple (multiplex). Growing down from the dermis with or without obvious connection is a cystic structure lined by a thick, refractile eosinophilic cuticle (Fig. 23.20). The remainder of the cyst wall consists of stratified squamous cells lacking a granular layer [71, 72]. In many cases, small sebaceous glands can be identified. Smooth muscle may be present in the wall of the cyst [71]. The cystic dilatation is believed to emanate from the junction at the insertion of the sebaceous duct into the follicular epithelium [69]. The diagnosis can be rendered with a high degree of certainty based solely on the lining cuticle and in the absence of readily identifiable sebaceous structures. The so-called hybrid cysts demonstrate features of steatocystoma adjacent to features of vellus hair cysts, and coexistence of both types of cysts has been described in some patients [73–76]. Diagnosis can be made on fine needle aspiration cytology specimens, but this is not the usual manner for establishing the diagnosis [77]. The presence of multiple steatocystomas has been associated with pachyonychia congenita. There are no differentiating characteristics based upon histologic presentation between sporadic lesions and those associated with the pachyonychia congenita [78, 79].
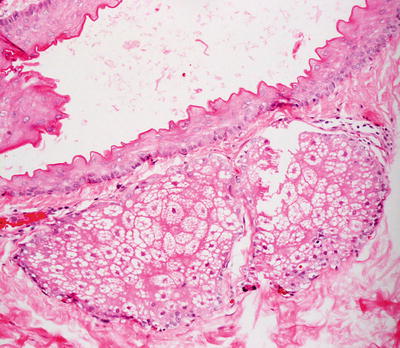
Fig. 23.20
Steatocystoma is characterized by epithelial lining with an eosinophilic cuticle and contains sebaceous glands within the cyst wall in some cases
23.11.3 Pathogenesis
Steatocystoma multiplex is a condition in which multiple steatocystomas are present. It has an autosomal dominant inheritance pattern [70]. However, numerous sporadic cases with no apparent genetic association have been reported. Mutations in the keratin-17 (K17) gene have been found in familial cases [80, 81]. Sporadic forms of the disease do not show associated K17 gene mutations. Keratin-17 is a type I keratin present in cutaneous appendages, such as the nail bed, hair follicles, and sebaceous glands. Steatocystoma multiplex has been found to be associated with pachyonychia congenita type II, and the same mutations in K17 have been described in both disorders, leading to the hypothesis that steatocystoma multiplex is a limited form of pachyonychia congenita type II [81].
23.12 Pilonidal Sinus
23.12.1 Clinical Features
Pilonidal sinus disease most often occurs in young men between 15 and 24 years of age [82]. It can occur in any ethnicity or race, but it is uncommonly seen in Asians and most frequently reported in hirsute Caucasians [83]. Pilonidal sinus disease is characterized by painful, intermittent swelling, erythema, and purulent draining of the superior gluteal cleft or sacrococcygeal area of the back [84]. The condition frequently is associated with an underlying cyst or sinus tract. Lesions often require surgical management [82].
23.12.2 Histology
The histologic changes seen in a pilonidal sinus are not specific. An epithelial-lined sinus tract is present, and in most cases appears ulcerated and inflamed. Isolated hair shafts may be observed within the sinus tract or in the adjacent dermis. Within the surrounding dermis, there is a dense inflammatory infiltrate that is diffuse and variable. In acutely inflamed cases, there is a brisk neutrophilic infiltrate, and eosinophils may be present. In less acute situations, a lymphohistiocytic infiltrate may be observed. In many cases, a granulomatous response is present with abundant multinucleated giant cells and mononuclear histiocytes. In these situations, keratinaceous debris is present within the giant cells .
23.13 Apocrine Nevus
23.13.1 Clinical Features
Apocrine nevi are uncommon benign tumors that may be congenital or acquired and appear as late as adulthood [85]. They are well-circumscribed, skin-colored nodules or pedunculated masses, ranging in size from 2 to 8 cm [86]. Lesions most commonly present at the axillae but can also occur on the scalp, sternum, and groin [85]. Apocrine nevi are primarily asymptomatic, although some individuals complain of associated tenderness, hyperhidrosis, alopecia, or draining. Malignant transformation has rarely been reported.
23.13.2 Histology
In apocrine nevus, the dermis contains mature apocrine glands that extend from the papillary into the reticular dermis. These glandular structures are often larger than normal apocrine glands, and may arise in sites not normally associated with apocrine glands (Fig. 23.21). Large eosinophilic cells with decapitation secretion into the luminal structures line the glandular structures (Fig. 23.22). There are no cytologic atypia and mitotic activity [86].
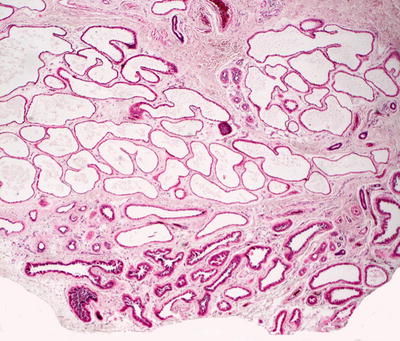
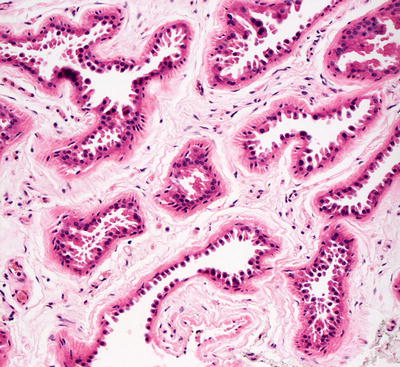
Fig. 23.21
The dermis is filled with abundant fully mature apocrine glands in an apocrine nevus
Fig. 23.22
Apocrine epithelium with typical hobnailing and eosinophilic cytoplasm is seen in apocrine nevus
23.14 Eccrine Nevus
23.14.1 Clinical Features
Eccrine nevus is an uncommon hamartoma comprised of an increased number and size of eccrine glands [87]. Eccrine nevus has a variable clinical presentation, but it is primarily characterized by localized hyperhidrosis [87]. Subtle brown hyperpigmentation has been described with overlying depressed area of skin, solitary sweat-discharging pore, and discrete papules. Spontaneous resolution has been described, although treatment of symptomatic cases can be difficult.
23.14.2 Histology
The histologic findings in an eccrine nevus are those of increased number and size of eccrine secretory coils within the mid-dermis (Figs. 23.23 and 23.24). The epidermis is usually unremarkable as is the surrounding dermis [88]. A polypoid configuration is sometimes described [89]. A porokeratotic eccrine nevus demonstrates similar findings, but the overlying epidermis is hyperkeratotic and acanthotic [90–92].
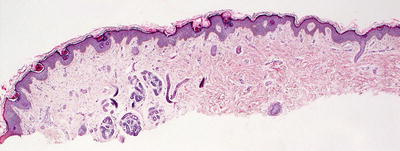
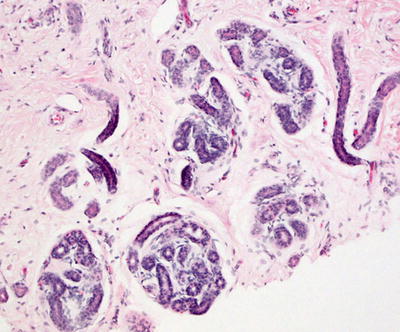
Fig. 23.23
A cluster of well-formed, fully mature eccrine structures characterizes eccrine nevus
Fig. 23.24
Eccrine nevus demonstrates increased numbers of mature eccrine structures
23.15 Eccrine Angiomatous Hamartoma
23.15.1 Clinical Features
Eccrine angiomatous hamartoma is an uncommon malformation characterized by hyperplasia of both eccrine and vascular structures [93]. Lesions may be congenital or present in early childhood, and rarely develop in adolescence or adulthood [93, 94].
Eccrine angiomatous hamartoma is described as a red to violaceous plaque, typically occurring on the distal extremity and may have associated pain, hyperhidrosis, and hypertrichosis. Lesions tend to expand proportionately to the child’s growth. Eccrine angiomatous hamartoma is benign, but may be surgically excised if symptomatic.
23.15.2 Histology
A biopsy specimen of eccrine angiomatous hamartoma demonstrates skin with a benign proliferation of eccrine ductules and glands within the mid-reticular dermis (Figs. 23.25 and 23.26) [95]. The epithelial structures are cytologically normal, and there is no keratinocyte proliferation within the excessive numbers of normal-appearing eccrine ducts and glands. Rare cases with verrucous epidermal hyperplasia have been described [96]. In these cases, the differential diagnosis includes verrucous hemangioma. There is also a proliferation of blood vessels of mixed size with varying amounts of muscle in the vessel walls [97]. The nature of the vessels is controversial with some authors claiming that the vessels are of lymphatic origin and others refuting this finding [98, 99]. The surrounding stroma is usually fibromyxoid with occasional cases demonstrating increased amounts of dermal mucin. Collagen bundles are thickened, haphazard in distribution, and may be perpendicular to the skin’s surface. Admixed adipocytes and neural structures are described in some cases [100].
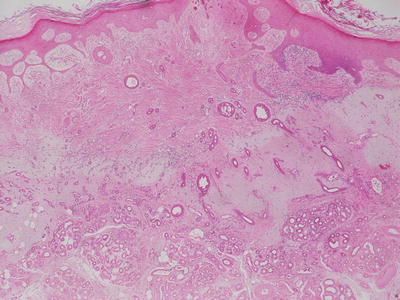
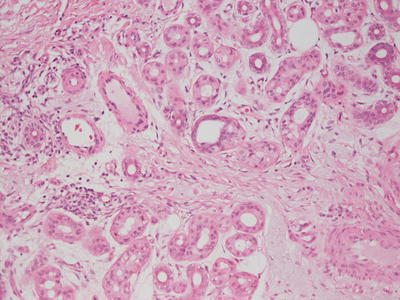
Fig. 23.25
Abundant well-formed eccrine structures and dermal blood vessels are present in the dermis in eccrine angiomatous hamartoma
Fig. 23.26
Eccrine angiomatous hamartoma has abundant well-formed eccrine structures admixed with thin- and thick-walled vessels
23.15.3 Pathogenesis
Eccrine angiomatous hamartoma is a benign growth of eccrine and vascular structures. Some authors believe that the lesion is primarily a vascular malformation with associated eccrine abnormalities [97, 98, 101]. A proposed model of the pathogenesis of congenital cases of eccrine angiomatous hamartoma describes the dysregulation of epithelial and mesenchymal tissues during embryonic development, leading to the abnormal proliferation of adnexal structures and blood vessels [97, 102].
23.16 Epidermal Nevus
23.16.1 Clinical Features
Epidermal nevi are usually present at birth or appear during early childhood. They occur with equal frequency in males and females [103]. Epidermal nevi present as hyperpigmented, clustered, velvety to verrucous papules or plaques arranged in a linear configuration (Fig. 23.27). They are most commonly seen on the extremities and typically distributed in a Blaschkoid pattern [103]. Lesions are usually solitary, although multiple lesions may occur. Epidermal nevi are benign tumors of epidermal structures. They may continue to expand but have no malignant potential. Treatment may be difficult and is dependent on the location, size, and patient preference.

Fig. 23.27
Epidermal nevus appears as a cluster of soft to slightly rough mamillated brown papules in a linear configuration along the lateral neck
23.16.2 Histology
There are several different histologic patterns that can be seen in these hamartomatous lesions. The histologic changes include hyperkeratosis and acanthotic epidermis (Figs. 23.28, 23.29 and 23.30). Hypergranulosis is seen in some cases, but it is not pronounced. The rete ridges are elongated. Cytologic atypia is not present, and mitotic activity is not increased.
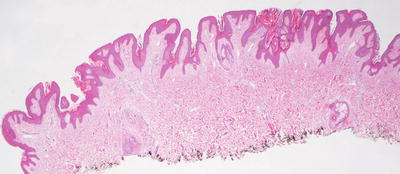
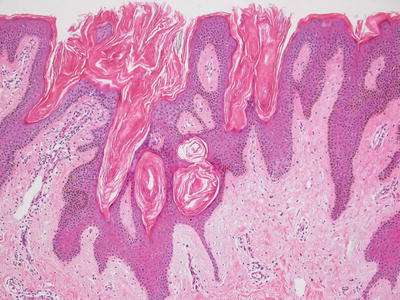
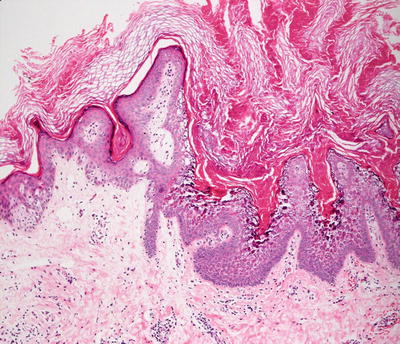
Fig. 23.28
An epidermal nevus has a papillomatous surface and acanthotic epidermis that is histologically indistinguishable from a seborrheic keratosis
Fig. 23.29
The epidermis is comprised of basaloid cells with focal horn cysts and overlying hyperkeratosis in epidermal nevus
Fig. 23.30




In some cases, changes of epidermolytic hyperkeratosis are seen in an epidermal nevus
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
