FIGURE 12.1 Acute versus cumulative irritation—a thought starter.
So what should be done in practice? Firstly, it is appropriate to adopt a protocol in which the skin exposure bears some resemblance to real-life exposure. Exposure may need to be repetitive, carried out for days, or even weeks. Next, it is essential to ensure that there is sufficient sensitivity built into the study to gain a meaningful response—a wholly negative set of skin reactions means nothing in isolation. Therefore, what is required is a panel with a sufficient number of volunteers and/or selection of panelists known to react with greater vigor to the type of irritancy problem associated with test material. It is almost always necessary to include a positive control material—a common choice is the anionic surfactant SLS, but it should generally be a last resort, since a better positive control is a related chemical or product formulation, relevant to the test material. For example, a clinical study of a new hand wash detergent formulation could involve several short exposures per day, with rinsing on one skin site, compared to a positive control site in which a product known to produce skin irritation in the exposed population is deployed. This study can then compare both the time to develop a cumulative irritant response, the nature and the degree of the irritant response, and as with all clinical studies, any observations on other aspects of the skin reaction, including sensory events. Ultimately, the question is “Does my clinical study have scientific integrity?”
There is one additional general question that has to be considered—how should any irritant reactions be assessed/measured? An argument can be made that properly trained skin assessors are more than sufficient to the task (14). However, and notwithstanding the additional time and expense, a good case can be made for use of one or (more usually) more instrumental assessment techniques (reviewed in the study by Berardesca and Maibach (15)).
Urticaria
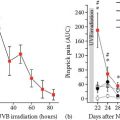
In the preceding sections, it has been documented that urticaria has little relationship to skin irritation. This should hardly be a surprising statement. The mechanisms driving the two reactions are not at all the same (even if we do not necessarily always know what those mechanisms are!). Irritation is largely some combination of damage to the skin barrier function together with the activation of inflammatory pathways and, even with the acute response, occurs over a time period measured in hours/days (16). Skin contact urticaria on the other hand (we are not speaking here of systemic disease types classed as urticaria) arises within a few minutes and typically fades over an hour or so. Commonly, two types of contact urticaria are described (17). Here, we will focus only on the nonimmunologic variety, avoiding the complexity of immunoglobulin E-mediated protein allergic responses.
Nonimmunologic contact urticaria is perhaps not only particularly common, but also relatively easy to screen for. A good number of common chemical urticants are known, and from these, valuable insights have been derived, if not into the precise mechanism(s) of action, at least into the general characteristics of the response (18). Firstly, almost all individuals will produce a typical erythematous response, perhaps with a wheal, a few minutes after skin contact with a strong urticant (e.g., ethyl nicotinate, dimethylsul phoxide [DMSO]). Weaker urticants (e.g., benzoic acid, sorbic acid) do not produce any reaction in many subjects, particularly at lower concentrations (17
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


