, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
14.1 Scabies
14.1.1 Clinical Features
Scabies is a common parasitic infestation of the skin caused by the mite Sarcoptes scabiei. Scabies affects individuals of all ages. Over 300 million cases are reported annually worldwide [1]. Clinically, patients experience intense pruritus and develop a cutaneous hypersensitivity reaction that manifests as a widespread eruption of erythematous papules and nodules [2] (Figs. 14.1 and 14.2). Vesicles and bullae may be seen. Upon close inspection of the skin, linear burrows can be detected as well. The hands, wrists, abdomen, and genitalia tend to be heavily involved. A crusted form may occur, manifesting as thick hyperkeratotic plaques and crusts particularly over the dorsal hands, feet, and extensor elbows and knees [3]. Therapy consists of topical and oral insecticides, and the prognosis is generally good, although post-scabies dermatitis may exist for weeks after the mite has been eliminated [2].


Fig. 14.1
Scabies presents as crusted erythematous, edematous papules scattered on the lower abdomen
Fig. 14.2
Similar crusted, erythematous papules are noted along the upper back in the same infant from Fig. 14.1
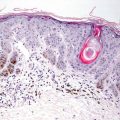
14.1.2 Histology
Biopsies from children with Sarcoptes scabiei infestations demonstrate changes of a dermal hypersensitivity reaction. Within the stratum corneum, small foci of parakeratosis and serum may be the first clue to the diagnosis. A spiky appearance to the epidermis has been described as a clue to the diagnosis [4]. Occasionally, mites or body parts from the mites may be identified within the stratum corneum, although frequently this requires study of multiple histologic levels [5] (Figs. 14.3 and 14.4). Some authors have advocated that a shave biopsy of the epidermis is the most sensitive method for detecting mites or their eggs, but this is not standard practice [6]. It is unusual to find organisms in the skin beneath the stratum corneum. The dermis contains a dense superficial and deep infiltrate of lymphocytes, histiocytes, and abundant eosinophils that may extend into the subcutaneous fat. Presence of germinal centers is not uncommon.
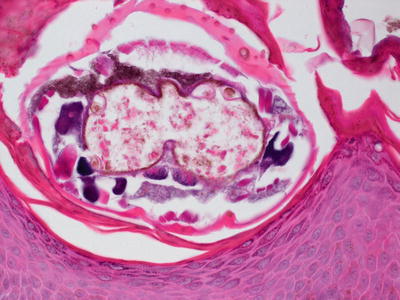

Fig. 14.3
Entire mites are readily observed at the base of the stratum corneum in some cases of scabietic infestation
Fig. 14.4
Scabies mite
Norwegian scabies, which are a rare variant that usually occurs in immunocompromised patients, are abundant and can be easily detected on routine sections (Figs. 14.5, 14.6 and 14.7). There is marked hyperkeratosis and epidermal acanthosis. Scabietic body parts are present diffusely throughout the stratum corneum [7, 8].
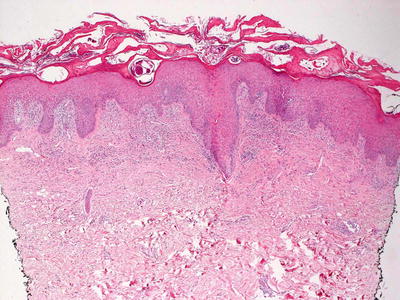
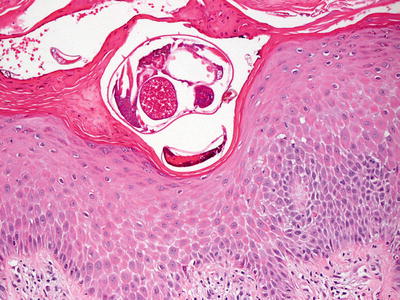
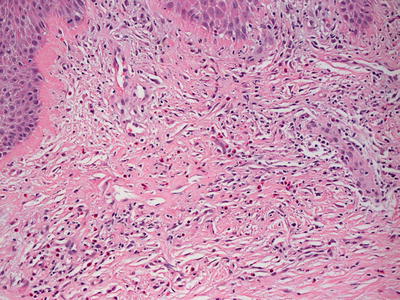
Fig. 14.5
Scabies are present within the stratum corneum in a case of Norwegian scabies. They are abundant and readily apparent on H&E stains
Fig. 14.6
Female mites are present within the stratum corneum in Norwegian scabies
Fig. 14.7
The dermis demonstrates a diffuse and dense inflammatory infiltrate with abundant eosinophils in Norwegian scabies
Persistent or nodular scabetic reactions that may remain after the organisms are treated can result in pronounced dermal inflammatory infiltrate. Abundant eosinophils are admixed with lymphocytes, and germinal centers may be present. The infiltrate is superficial and deep and may be peri-appendageal. In some cases, lymphoma may be in the differential diagnosis [9]. A lymphocytic vasculitis has been reported in rare cases, although this is not a common finding [10]. Enlarged lymphocytes with cytologic atypia are described in persistent scabietic nodules. These cells may express CD30, resulting in further diagnostic overlap with T cell dyscrasias, such as lymphomatoid papulosis [11].
The histologic differential diagnosis of scabies infection includes Langerhans cell histiocytosis . This is due to the abundance of intraepidermal Langerhans cells present as a reaction to scabietic mite, as well as to the eosinophilia within the dermis. However, presence of organisms and a marked inflammatory infiltrate enable distinction in most cases [12, 13]. Acropustulosis of infancy may also present a diagnostic challenge, but this entity is usually neutrophil predominant, and it does not display intense eosinophilia [14]. Some authors believe there is a relationship between infantile acropustulosis and scabietic infestation [15]. Eosinophilic pustular folliculitis is also a differential consideration, but this is not a specific histologic finding, but rather a reaction pattern that can be seen in patients with scabies infestation [16].
14.1.3 Pathogenesis
Sarcoptes scabiei is transmitted by person-to-person contact. Female mites lay up to three eggs per day in skin burrows in the epidermis. The larvae hatch into nymphs, from which adult males or females emerge in 10–14 days. Inactivated serine proteases and glutathione S-transferases from scabies mites are important immunogenic antigens [17, 18]. Inactivated serine proteases act as inhibitors of inflammation, thus protecting scabies mites from the host inflammatory response [19]. Scabies infestation results in delayed type-IV hypersensitivity reaction against mites and mite-product antigens with a latency period of up to 4 weeks, during which time the patient is asymptomatic [19].
14.2 Spider Bites
14.2.1 Clinical Features
There are more than 30,000 species of spiders, but most cannot or do not inflict serious bites to humans [20]. There are two medically important spiders in the United States: the black widow ( Latrodectus mactans ) and the brown recluse ( Loxosceles reclusa ).
The black widow spider is identifiable by a red hourglass marking on its ventral abdomen. The venom of a black widow spider mainly causes severe crampy muscle spasms and no significant or diffuse cutaneous changes [21].
The brown recluse spider bite, however, has the potential to cause significant skin necrosis. Typically, a tender erythematous patch or edematous plaque develops at the site of the bite, occasionally with concomitant pain at the time of injury (Fig. 14.8). The majority of bites heal within 3 weeks without significant complications [22]. In 40 % of cases, an expanding area of necrosis develops, and 10–15 % of patients will experience significant scarring [20, 21].

Fig. 14.8
Spider bite shows well-circumscribed ulceration with surrounding irregularly shaped, edematous erythema
Black widow bites are treated with antivenom, as well as pain control and benzodiazepines for muscle spasms. Brown recluse bites are treated with local wound care. Dapsone treatment is controversial, but may be helpful in some cases [21].
14.2.2 Histology
Spider bites induce a characteristic, but not specific histologic reaction pattern. Vascular destruction in the mid to deep reticular dermis results in a large area of dermal necrosis, and overlying epidermal ulceration (Figs. 14.9 and 14.10). This coagulative necrosis has been described as “mummified necrosis” [23]. Transmural inflammation of vessel walls gives rise to local vasculitis involving medium-sized dermal vessels. This pattern can resemble that seen in polyarteritis nodosa, but this is a localized phenomenon [23]. The necrosis can be extensive and destructive [24]. There is a diffuse and dense mixed inflammatory infiltrate in the dermis. Abundant neutrophils may be present in the regions with necrosis, resulting in an eosinophilic cellulitis appearance in some cases [25].
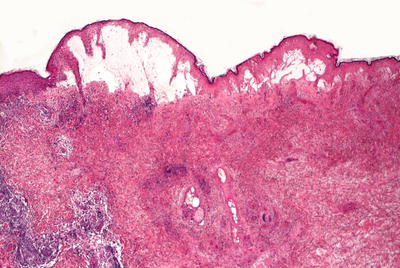
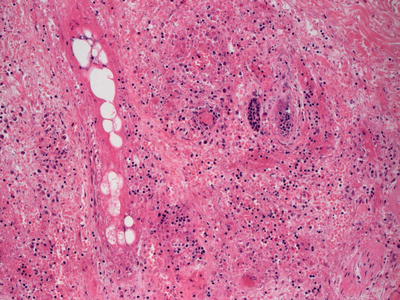
Fig. 14.9
Spider bites demonstrate epidermal necrosis, vascular thrombosis, and a dense and diffuse inflammatory infiltrate
Fig. 14.10
Thrombosed vessels give rise to necrotic dermis and karyorrhectic debris in spider bites
Lymphohistiocytic hematophagocytosis and severe hemolytic anemia have been described as a consequence of spider bites [26, 27]. Erythema multiforme and acute generalized exanthematous pustulosis (AGEP) reaction patterns have been described in patients with spider bites [28, 29]. Lyme disease can enter the differential diagnosis [30]. However, the inflammatory infiltrate in Lyme disease is far less intense in most cases, and overt vascular destruction is extremely uncommon .
14.2.3 Pathogenesis
Spiders that can cause serious injuries to people include the funnel web spider of Australia (genus Atrax), armadeira spider (genus Phoneutria), black widow spider (genus Latrodectus), and brown recluse spider (genus Loxosceles). The first three spiders release neurotoxin that can cause serious injuries and even death, with little or no skin changes [31]. Black widow spider (Latrodectus mactans ) causes intense pain at the bite site. The spider venom contains α-latrotoxin, which causes the release of catecholamine from nerve synaptic terminals [32, 33]. Clinical symptoms resulting from this spider bite include severe muscle spasms, tachycardia, high blood pressure, agitation, and pain [34]. Brown recluse spider (Loxosceles reclusa ) bites, by contrast, cause marked skin changes from local tissue injury. The venom of the brown recluse spider contains enzymes that cause tissue damage. Key enzymes in the venom are sphingomyelinase D and hyaluronidase [34–36]. These enzymes cause damage to blood vessel walls and red blood cells, leading to extensive tissue damage and necrosis. In about 5 % of cases, hemolysis from red blood cell damage leads to acute kidney failure [36, 37]. Hyaluronidases also degrade extracellular matrix components, and increase the diffusion of other toxins from the inoculation site [38].
Proteomic analysis of brown spider venom revealed a number of toxins generally found in animal venoms, and are believed to cause tissue damage in loxoscelism [39]. Among these, phospholipase D (PLD) is a key enzyme in spider venom. PLD enzymatic activity leads to dermal necrosis in vivo, making it a dermal necrotic toxin [38]. Mechanistically, PLD hydrolyzes cell membrane sphingomyelin to ceramide 1-phosphate, leading to an exuberant inflammatory response [40]. There are at least 11 isoforms of PLD in the venom of Loxosceles [39]. There are two PLD isoforms from Loxosceles (class I and class II phospholipase D), which cause complement-dependent hemolysis, dermal necrosis and hydrolysis of sphingomyelin [41, 42].
Besides PLD, other key enzymes in Loxosceles spider toxins are metalloproteases, hyaluronidases, TCTP (Translationally Controlled Tumor Protein ) member family toxin, and Inhibitor Cystine Knot peptide from brown spider venom [38].
14.3 Tick Bites
14.3.1 Clinical Features
Ticks are arachnids that serve as hosts and vectors of human infectious diseases. Tick parts embedded in human skin may cause local acute erythematous lesions or chronic granulomatous response. Rarely, tick bites can lead to panniculitis, vesicles and hemorrhage. Complete removal of all tick parts is important to minimize adverse cutaneous sequela. Erythema chronicum migrans is a cutaneous manifestation of Lyme disease from the bite of hard ticks of the genus Ixodes, and it is described elsewhere in this volume. Likewise, Rocky Mountain spotted fever is also a tick-borne disease with cutaneous manifestations that is addressed elsewhere.
14.3.2 Histology
The local cutaneous reaction to a tick bite is essentially a dermal hypersensitivity reaction, not unlike arthropod bite reactions. In some cases, tick body parts can be identified within the epidermis, especially the stratum corneum (Fig. 14.11 and 14.12). Within the dermis, there is a brisk inflammatory response of neutrophils, lymphocytes, and often abundant eosinophils. When present, the reaction pattern is that of Wells syndrome or eosinophilic cellulitis [25]. The infiltrate is superficial, deep and diffuse, and may extend into the subcutaneous fat. Endothelial cell swelling has been described within dermal vasculature and extravasation of erythrocytes is common [43]. A granulomatous response to actual tick parts has been described, but it is not commonly encountered [43]. Eosinophilic deposits that resemble cryoglobulins have been described in tick bite reactions [44]. In some cases, florid cutaneous lymphoid hyperplasia arises at the site of a tick bite [45]. In rare situations, the dermal lymphocytes may have cytologic atypia and express CD30, giving rise to concern for lymphoma [46–48].
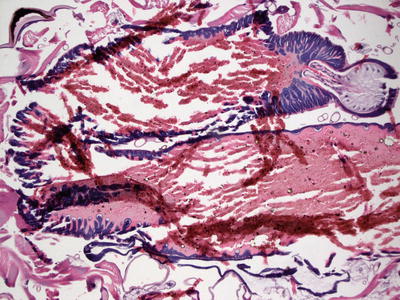
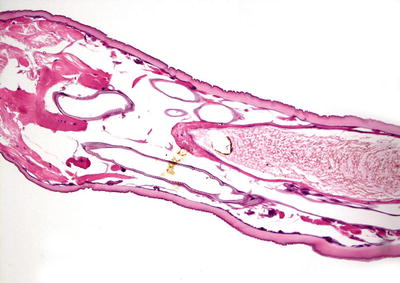
Fig. 14.11
Histologic sections demonstrate the anatomic structures characteristic of a tick
Fig. 14.12
A thick eosinophilic cuticle is observed surrounding internal structures in a tick
14.4 Lice
14.4.1 Clinical Features
Pediculosis capitis or head lice is caused by the insect Pediculus humanus capitis . Head lice infestation affects 6–12 million children in the United States annually [49, 50]. Most affected individuals are between 3 and 11 years of age, since this population has higher rates of head-to-head contact with their peers and more often share hair utensils and garments [50]. Head lice are least likely to affect African-Americans. Clinical findings in the scalp hair include numerous live lice and egg cases (“nits”), which are firmly adherent to the hair shafts within a few millimeters of the scalp (Fig. 14.13). Another kind of body lice that are commonly found worldwide are crab lice or pubic lice. These are parasitic insects found mainly in hair-bearing genital/pubic area (Fig. 14.14).


Fig. 14.13
Head louse nits are often found on hairs in children (photograph courtesy of Eric Rosenbaum, MD, University of Arkansas for Medical Sciences)
Fig. 14.14
The characteristic shape of a crab louse is easily identified when the organism is submitted intact for processing
14.4.2 Histology
Infestation with lice rarely requires biopsy diagnosis as organisms and their eggs are grossly apparent [52]. When a biopsy is performed, chitinous arthropod may be seen within the stratum corneum and epidermis. If the entire organism is present, erythrocytes may be found in the insect gut, and insect striated muscle is apparent. The dermis demonstrates a dermal hypersensitivity reaction with a diffuse and dense polymorphous inflammatory infiltrate, often with abundant eosinophils [53]. Overlying excoriation is common due to intense pruritus [54]. In rare cases, lymphocytes within the dermal infiltrate may be cytologically atypical and express CD30, thus giving rise to concerns for cutaneous lymphoma [55].
14.4.3 Pathogenesis
Head lice are ectoparasites that live in the scalp and feed on human blood. Racial predilection purportedly exists due to the inability of the louse to attach to particular hair types [50]. Adult lice are 2–3 mm long with elongated, flattened torsos, and they do not have wings. Lice eggs are glued to the hair shaft close to the scalp. The warmth and moisture of the scalp help incubate the eggs, which hatch into nymphs in 6 to 10 days [56]. The nymphs molt several times over 9 to 12 days and become adult lice. Body lice are known to transmit bacteria that cause epidemic typhus (Rickettsia prowazekii ), louse-borne relapsing fever (Bartonella recurrentis), and trench fever (Borrelia quintana ) [57].
14.5 Cutaneous Larva Migrans
14.5.1 Clinical Features
Cutaneous larva migrans is a pruritic zoodermatosis caused by penetration of the skin by larvae of animal hookworms. Eggs are deposited in the soil via the feces of infested dogs and cats. Humans become infected by contact with contaminated soil, often while going barefoot or sitting on the ground wearing shorts or swimsuits. Ancylostoma braziliense is the hookworm species that most commonly affects humans [58]. Lesions are characterized by intensely pruritic, erythematous, linear or serpiginous plaques, often located on the feet, ankles, posterior thighs, and buttocks [59] (Fig. 14.15).

Fig. 14.15
Cutaneous larva migrans presents as serpiginous plaque at the ankle
Cutaneous larva migrans typically heals spontaneously within weeks to months. However, given the intense pruritus and potential for secondary infection due to scratching, treatment is warranted. Although a variety of methods have been reported, the most effective treatments are topical or oral anti-helminthic agents, such as thiabendazole and ivermectin .
14.5.2 Histology
Cutaneous larva migrans caused by toxocariasis seldom needs to be biopsied [60]. Routine sections reveal a superficial and deep perivascular inflammatory infiltrate with lymphocytes and scattered eosinophils. Neutrophils are also present in most cases, and plasma cells may be seen in some cases. Dermal edema giving rise to the appearance of urticaria is common. In some cases, the burrowing tunnels can be seen in the epidermis, but this is usually quite difficult to appreciate. When present, they appear as round to oval spaces within the epidermis [4]. In most cases, the histologic findings are not diagnostic. On rare occasions, the larvae can be seen within the epidermis and occasionally within cutaneous appendages [61]. Lesions may resolve with post-inflammatory hyperpigmentation that can be diagnosed on biopsy, but without any possibility of attribution for the antecedent condition [62].
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


